Clinical Image
Andy Gump deformity

Pirabu Sakthivel1*, Chirom Amit Singh2, and Suresh Chandra Sharma3
1Department of Otorhinolaryngology & Head and Neck surgery, All India Institute of Medical Sciences, New Delhi, India
2Department of Otorhinolaryngology & Head and Neck surgery, All India Institute of Medical Sciences, New Delhi, India
3Department of Otorhinolaryngology & Head and Neck surgery, All India Institute of Medical Sciences, New Delhi, India
*Address for Correspondence: Pirabu Sakthivel, M.S., DNB. ENT, Department of Otorhinolaryngology & Head and Neck Surgery, All India Institute of Medical Sciences, New Delhi-110029, India, Tel: 9958744547, Email: [email protected]
Dates: Submitted: 21 August 2017; Approved: 21 September 2017; Published: 22 September 2017
How to cite this article: Sakthivel P, Singh CA, Sharma SC. Andy Gump deformity. J Clin Med Exp Images. 2017; 1: 046-047.
DOI: 10.29328/journal.jcmei.1001008
Copyright License: © 2017 Sakthivel P, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
A 63 year old gentleman presented with ulcer over the lower alveolus for the past 4 months duration. The patient also had pain, loose lower central incisors and occasional bleeding from the ulcer while brushing. On examination an ulceroproliferative growth was seen involving lower alveolus along with adjoining mucosa of the lower lip with mobile central incisors. There was associated bilateral submandibular area lymphadenopathy. Histopathological examination of the ulcer revealed moderately differentiated squamous cell carcinoma. The patient underwent wide local excision with central arch resection of mandible with bilateral modified neck dissection and pectoralis major myocutaneous flap for reconstruction followed by postoperative radiotherapy. During the follow up, patient developed severe “Andy Gump deformity” [Figure 1]. Surgical reconstruction was offered to the patient but denied consent for further intervention.
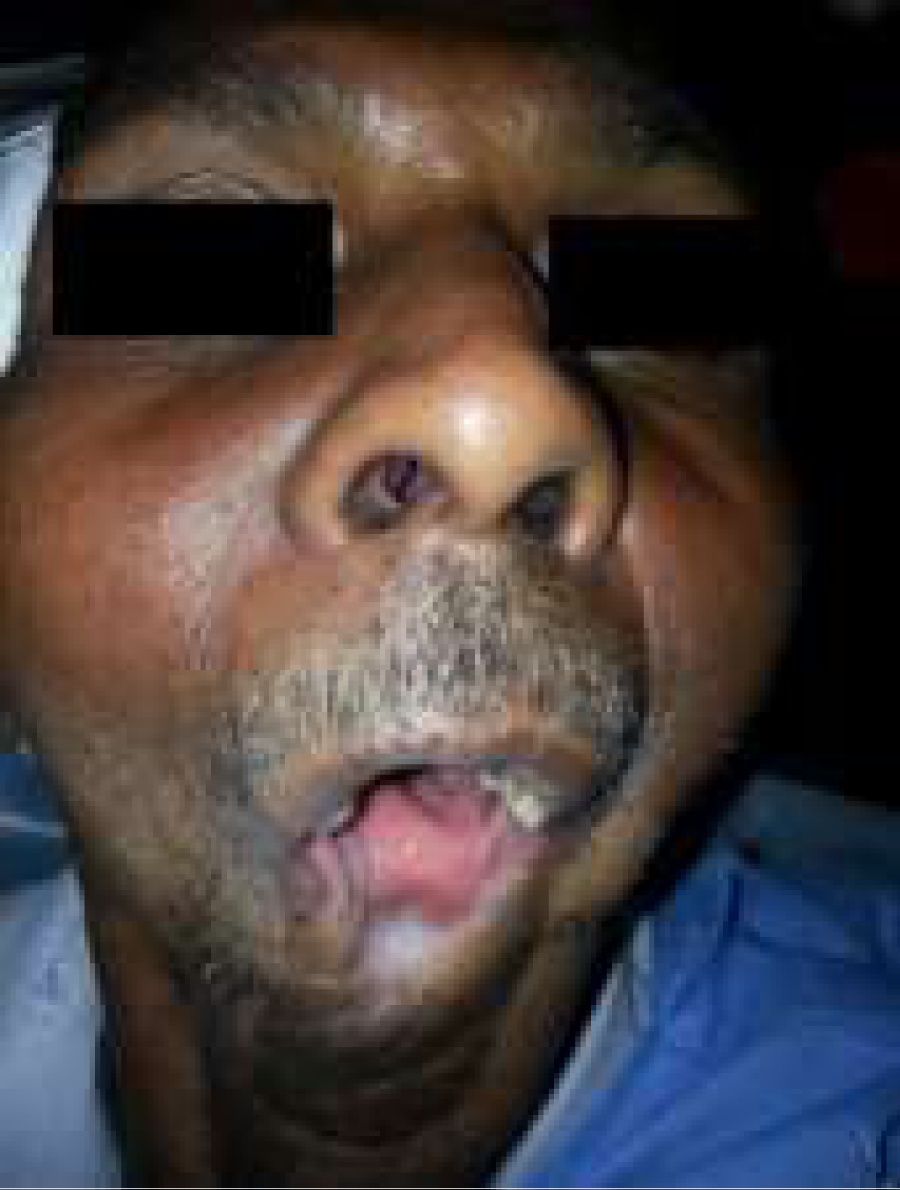
Figure 1: Clinical image showing the classical “Andy Gump deformity”. Note the drooling with mastication difficulty.
The “Andy Gump deformity” is a euphemism for an anterior mandibular defect that creates the appearance of an absent chin and lower lip and severely retrognathic lower jaw, which is named after a character in an early 20th-century comic strip [1]. Head and neck ablative surgery is the most common cause for this deformity [2]. Patients with this deformity are at risk for airway compromise, cosmetic embarrassment, excessive drooling, mastication difficulties, and speech impairment. Although reconstruction is difficult, with the use of vascularized bone flaps the deformity can corrected with more success [1].
Reference
- Aziz SR. Andy Gump and his deformity. J Oral Maxillofac Surg. 2010; 68: 651-653. Ref.: https://goo.gl/V9U3i2
- Seshul MB, Sinn DP, Gerlock AJ Jr. The Andy Gump fracture of the mandible: a cause of respiratory obstruction or distress. J Trauma. 1978; 18: 611-612. Ref.: https://goo.gl/dco3YS