
More Information
Submitted: March 15, 2021 | Approved: March 17, 2021 | Published: March 18, 2021
How to cite this article: Chen CC, Tsai HW, Hu SY. Aortic dissection complicating carotid dissection and myocardial infarction. J Clin Med Exp Images. 2021; 5: 003-003.
DOI: 10.29328/journal.jcmei.1001019
Copyright License: © 2021 Chen CC, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Aortic dissection complicating carotid dissection and myocardial infarction
Chun-Cheng Chen1, Hung-Wen Tsai2 and Sung-Yuan Hu1,3-5*
1Department of Emergency Medicine, Taichung Veterans General Hospital, Taiwan
2Division of Cardiovascular Surgery, Center of Cardiovascular Medicine, Taichung Veterans General Hospital, Taiwan
3School of Medicine, Chung Shan Medical University, Taiwan
4Institute of Medicine, Chung Shan Medical University, Taiwan
5Department of Nursing, College of Health, National Taichung University of Science and Technology, Taichung, Taiwan
*Address for Correspondence: Sung-Yuan Hu, Department of Emergency Medicine, Taichung Veterans General Hospital, 1650 Taiwan Boulevard Sect. 4, Taichung 40705, Taiwan, Tel: +886 4 23592525; ext 3601; Fax: +886 4 23594065; Email: [email protected]
A 58-year-old hypertensive man presented to our insti-tution with acute chest pain and dizziness. Electrocardiogram revealed inferior wall myocardial infarction with suspected right ventricular involvement (Figure 1A). Computed tomographic aortography (CTA) depicted ascending aortic dissection (AAD) with involvement of bilateral carotid, subclavian, and right common iliac arteries (Figure 1B). Replacements of aortic valve and ascending aorta with CABG (Ao-RSVG1-LAD and Ao-RSVG2-RCA) were conducted.
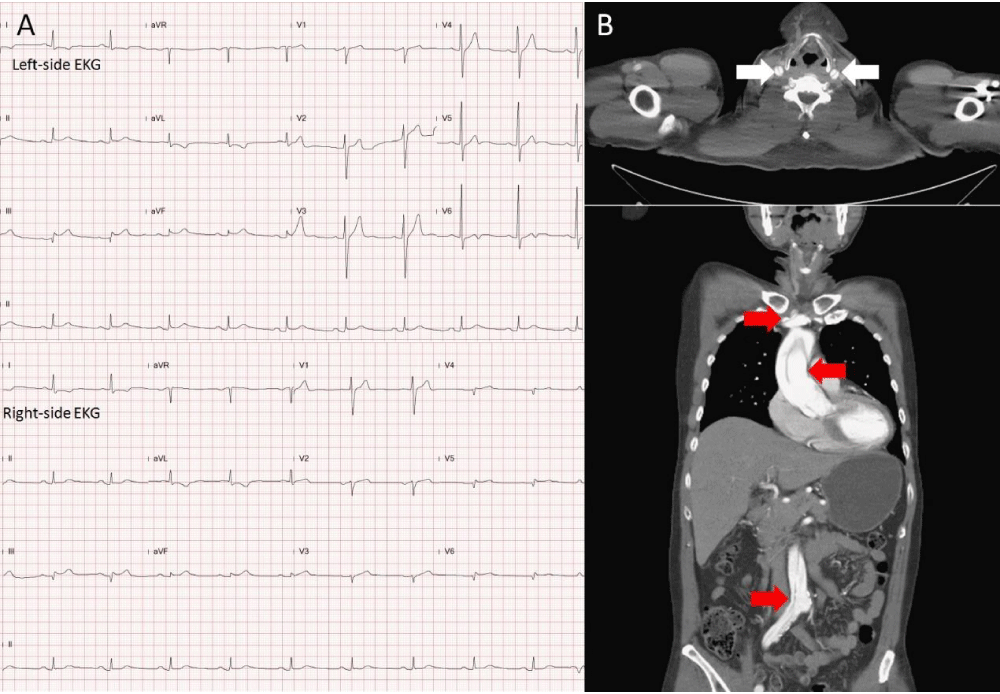
Figure 1: Left-side electrocardiogram (EKG) revealed ST-segment elevation in II, III, and aVF, with reciprocal changes in I and aVL, disclosing inferior wall myocardial infarction. Right-side (EKG) showed ST-segment elevation in V4, disclosing right ventricular involvement (Figure 1A). The axial and coronary views of computed tomographic angiography demonstrated dissection of bilateral carotid arteries (white arrows in Figure 1B) and dissection of ascending aorta with extending to subclavian and right common iliac arteries (red arrows in Figure 1B).
There are 5% - 8% of ST-segment elevation and 15% - 41% with dissection of the common carotid or subclavian artery in AAD [1-3]. CTA is a mandatory tool to confirm the diagnosis of AAD and its involvement [1]. Point-of-care ultrasound is an alternative tool to diagnose AAD if it is contraindicated or not available. AAD with involvement of coronary artery will lead to poor prognosis if delay intervention [1].
This study was approved by the Institutional Review Board of Taichung Veterans General Hospital (No. CE19152A).
This work was supported by grants from the Taichung Veterans General Hospital (Grant numbers: TCVGH-109 7202C). The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
- Alsaad AA, Odunukan OW, Patton JN. Ascending aortic dissection presented as inferior myocardial infarction: a clinical and diagnostic mimicry. BMJ Case Rep.2016; 20: bcr2016217543. PubMed: https://pubmed.ncbi.nlm.nih.gov/27999129/
- Chen A, Ren X. Aortic Dissection Manifesting as ST-Segment-Elevation Myocardial Infarction. Circulation. 2015; 131: e503-504. PubMed: https://pubmed.ncbi.nlm.nih.gov/26015467/
- Deniz T, Dag E, Tulmac M, Azapoglu B, Alp C. What Lies behind the Ischemic Stroke: Aortic Dissection? Case Rep Emerg Med. 2014; 2014: 468295. PubMed: https://pubmed.ncbi.nlm.nih.gov/25544904/