
More Information
Submitted: February 13, 2026 | Accepted: February 18, 2026 | Published: February 19, 2026
Citation: Mamad A, Bibat MA, Elafari MA, Moncef M, Slaoui A, Karmouni T, et al. Stone on the Mesh: Intravesical Erosion after Laparoscopic Promontofixation-A Hidden Cost of Durability. J Clin Med Exp Images. 2026; 10(1): 006-009. Available from:
https://dx.doi.org/10.29328/journal.jcmei.1001040.
DOI: 10.29328/journal.jcmei.1001040
Copyright license: © 2026 Mamad A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Promontofixation; Mesh erosion; Intravesical erosion; Bladder calculus; Cystoscopy

Stone on the Mesh: Intravesical Erosion after Laparoscopic Promontofixation-A Hidden Cost of Durability
Ayoub Mamad* , Mohammed Amine Bibat, Mohammed Amine Elafari, Midaoui Moncef, Amine Slaoui, Tarik Karmouni, Abdelatif Koutani and Khalid Elkhader
, Mohammed Amine Bibat, Mohammed Amine Elafari, Midaoui Moncef, Amine Slaoui, Tarik Karmouni, Abdelatif Koutani and Khalid Elkhader
Urology B Department, IBN Sina Hospital, University Hospital Center IBN SINA, University Mohammed V, Rabat, Morocco
*Corresponding author: Ayoub Mamad, Urology B Department, IBN Sina Hospital, University Hospital Center IBN SINA, University Mohammed V, Rabat, Morocco, Email: [email protected]
Intravaginal erosion of synthetic mesh after laparoscopic promontofixation(sacrocolpopexy) is an uncommon but clinically relevant late complication. When mesh becomes exposed within the bladder, it may function as a persistent foreign body, encouraging chronic inflammation, bacterial colonization, recurrent lower urinary tract symptoms, and progressive encrustation that can culminate in bladder stone formation. We report a 60-year-old woman with a history of laparoscopic promontofixation using standard polypropylene mesh performed approximately five years earlier. She presented with progressive urinary symptoms. Bladder ultrasound demonstrated an intravesical calculus, and diagnostic cystoscopy confirmed a bladder stone developing on exposed intravesical mesh fibers, consistent with intravesical mesh erosion. Endoscopic management was performed with cystolithotripsy followed by section/resection and removal of the exposed intravesical mesh to eliminate the lithogenic nidus, with a favorable outcome. In women with prior promontofixation presenting with bladder stones, recurrent urinary tract infections, hematuria, or persistent irritative urinary symptoms, intravesical mesh erosion must be considered. Cystoscopy is essential for diagnosis because imaging may identify the stone but not the underlying foreign-body etiology, and definitive treatment requires both stone clearance and elimination of intravesical foreign material to prevent recurrence.
Laparoscopic promontofixation (sacrocolpopexy) is regarded as a durable reconstructive option for apical pelvic organ prolapse, providing long-term anatomic support and restoration of vaginal axis. Its success depends on fixation of a graft, most commonly polypropylene mesh, between the vagina and the sacral promontory. Despite excellent durability, mesh-related complications may occur, including erosion into adjacent organs such as the bladder [1,2]. Although the overall risk is low, intravesical mesh exposure has a disproportionate clinical impact because the mesh becomes bathed in urine and functions as a foreign body, potentially causing chronic inflammation, bacterial colonization, recurrent urinary tract symptoms, and stone formation [1-3]. Reported erosion rates vary with technique, length of follow-up, and associated procedures such as concurrent hysterectomy type [3,4]. Because urinary symptoms are common in the age group that undergoes prolapse surgery, intravesical erosion may be overlooked or misattributed to recurrent cystitis or overactive bladder, delaying definitive diagnosis. Timely recognition matters, since persistent intravesical foreign material can lead to recurrent encrustation and stone recurrence, and may require more complex intervention if extensive [1,2].
A 60-year-old woman, previously treated with laparoscopic promontofixation using a standard polypropylene mesh approximately five years earlier, presented with progressively worsening lower urinary tract symptoms. She reported irritative complaints, including urinary frequency, urgency, and dysuria, with occasional suprapubic discomfort. There was no history of recent pelvic trauma. Physical examination was unremarkable, and pelvic examination did not show signs of acute infection or vaginal mesh exposure.
Initial evaluation included urinalysis and bladder ultrasound. Ultrasound demonstrated an intravesical calculus without upper urinary tract dilatation. Given the history of prior mesh-based prolapse repair and the presence of a bladder stone, diagnostic cystoscopy was performed to identify a potential intravesical foreign body. Cystoscopy revealed a vesical calculus adherent to exposed mesh fibers protruding into the bladder lumen, confirming intravesical erosion of the promontofixation mesh (Figure 1). The surrounding bladder mucosa appeared inflamed at the contact site.
Endoscopic management was undertaken. Cystolithotripsy was performed to fragment and evacuate the stone. Following stone clearance, the exposed intravesical mesh segment was resected and removed endoscopically to eliminate the lithogenic nidus. Hemostasis was ensured, and the bladder was inspected at the end of the procedure to confirm complete stone removal and absence of residual intravesical foreign material. The postoperative course was favorable, with improvement of urinary symptoms during follow-up.
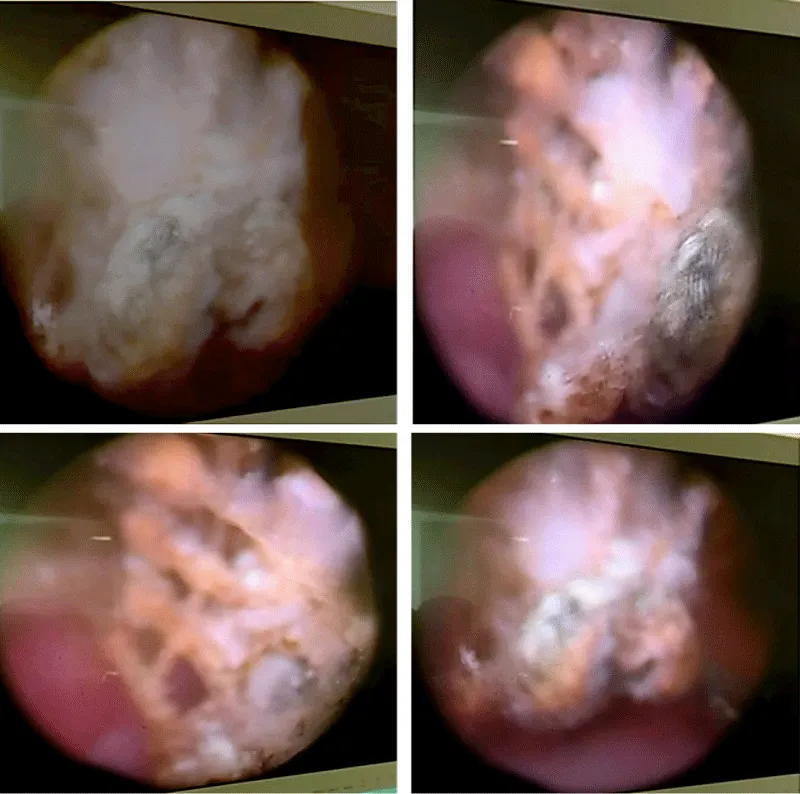
Figure 1: Cystoscopic view showing a bladder stone formed on exposed intravesical mesh fibers.
Bladder stone formation on eroded mesh is a classic expression of foreign-body lithogenesis. Once a synthetic material is exposed within the bladder lumen, it provides a surface for initial crystal adherence. Over time, this process is amplified by local inflammation and bacterial colonization, which can further promote deposition and encrustation [1,2]. In addition, the foreign surface may serve as a scaffold for biofilm formation, allowing bacteria to persist despite antibiotic therapy and perpetuating a cycle of chronic irritation and recurrent infection. When urease-producing organisms are involved, urinary alkalinization and precipitation of infection-related crystals may accelerate encrustation. However, stones may also form in the absence of such bacteria through progressive mineral deposition. Clinically, the patient may experience recurrent lower urinary tract symptoms, episodic hematuria, or recurrent urinary tract infections; alternatively, symptoms may remain subtle until a stone becomes large enough to produce overt irritative complaints or recurrent infection. Because these symptoms overlap with common benign conditions, clinicians may repeatedly treat presumed cystitis without identifying the underlying etiology, allowing the intravesical foreign body to persist and the stone burden to progress. In practice, repeated short-lived improvement with antibiotics, persistent sterile pyuria, or culture-negative “cystitis-like” symptoms should prompt consideration of a structural cause, particularly in patients with a history of pelvic mesh surgery.
A key diagnostic principle is that imaging and endoscopy play complementary roles, but cystoscopy is decisive. Ultrasound can detect an intravesical calculus, and CT (where available) can further define stone burden and anatomy; however, neither modality reliably proves mesh erosion or defines the exact extent of intravesical exposure. Imaging may also miss early or small exposures, especially if there is limited calcification. Furthermore, a calculus may appear “primary” on imaging, obscuring the causative foreign body. Cystoscopy provides direct visualization of the bladder mucosa and any foreign material, confirms the diagnosis, localizes the erosion, and guides treatment planning [1,2]. It also allows assessment of mucosal inflammation, ulceration, or localized granulation tissue, which may explain hematuria and irritative symptoms. Importantly, cystoscopy supports exclusion of alternative diagnoses that can coexist or mimic presentation, including bladder tumors, chronic inflammatory lesions, or other foreign bodies such as non-absorbable sutures. In practical terms, when a patient with a history of promontofixation presents with persistent urinary symptoms or a bladder stone, cystoscopy should be strongly considered even if cultures are intermittently negative or imaging appears to show only a “simple stone,” because the underlying cause may be a foreign body rather than primary stone disease.
Therapeutic success depends on addressing both the consequence (the stone) and the cause (the intravesical foreign body). If the calculus is removed but the exposed mesh is left behind, the foreign material continues to act as a nidus for renewed crystallization, making recurrence likely and leaving the patient at ongoing risk for symptoms and infection. Therefore, management must include stone fragmentation/removal plus elimination or ablation of the intravesical mesh segment [1,2]. This principle is central to counseling: patients should understand that symptom recurrence is expected if the intravesical exposure persists, even if initial stone removal provides temporary relief.
The choice of technique should be individualized to the extent of erosion, accessibility of exposed material, stone size, and local expertise. Endoscopic methods can be effective when the eroded component is limited and reachable, offering the advantages of minimal invasiveness, reduced morbidity, and quicker recovery. In the present case, endoscopic cystolithotripsy combined with resection of the exposed intravesical mesh successfully removed both the stone and the lithogenic nidus. Endoscopic removal may be performed using mechanical instruments or energy devices, depending on availability and the surgeon’s experience, but the goal remains complete elimination of intravesical foreign material while minimizing thermal injury to the adjacent bladder wall. When exposure is extensive, when mesh is deeply embedded, or when endoscopic access is incomplete, a transabdominal approach may be required to achieve definitive removal and bladder repair. A systematic review focused on surgical techniques for erosive mesh in the urethra and bladder supports that both cystoscopic and transabdominal approaches can be effective for bladder erosions, and that selection should be guided by the extent and accessibility of the eroded material.
Management decisions also require awareness of broader clinical trade-offs. Complete mesh excision may be technically challenging and can carry the risk of urinary tract injury, fistula formation, bleeding, or infection, and may affect pelvic support depending on how much supportive material must be removed. Inflammation around the erosion site can obscure tissue planes, and chronic encrustation may make dissection more difficult. Expert reviews and consensus-oriented guidance stress individualized planning, often in experienced centers, because these procedures require careful judgment and meticulous technique [1,2]. In addition, patients should be counseled that although addressing the intravesical complication is the priority, mesh excision may theoretically influence the durability of the original prolapse repair, and postoperative monitoring should include attention to both urinary outcomes and pelvic floor support. Follow-up should also consider recurrence prevention, including reassessment if symptoms return, because re-exposure or residual intravesical fibers, however small, may restart encrustation [5].
The timing of presentation in this case, approximately five years after promontofixation-reinforces that intravesical erosion may be a late complication. This is consistent with published experience, including a technique report describing management of intravesical erosion five years after laparoscopic promontofixation, supporting the timeframe and emphasizing the need to consider this diagnosis long after the initial surgery [6]. Late presentation may reflect gradual tissue attenuation, chronic mechanical stress, or a slow process of micro-exposure that becomes clinically apparent only once encrustation and calculus formation have progressed. Patient-related factors that impair tissue healing or resilience, such as hypoestrogenism, smoking, diabetes, or prior pelvic surgery, may contribute, as may procedure-related factors such as dissection close to the bladder wall or an unrecognized intraoperative injury [1,2].
From a preventive perspective, variability in reported erosion rates and the influence of concomitant hysterectomy type highlight that risk is multifactorial [3,4]. This underscores the importance of careful surgical technique, meticulous tissue handling, attention to bladder integrity during dissection, and long-term follow-up. Prevention also includes maintaining a low threshold to investigate postoperative urinary symptoms rather than treating recurrent episodes empirically. While no strategy eliminates risk, sustained awareness by both clinicians and patients can shorten diagnostic delay and reduce the likelihood of a large stone burden at presentation. Practically, clinicians should consider intravesical mesh erosion in any patient with a history of promontofixation who presents with a bladder stone, recurrent urinary tract infections, persistent irritative urinary symptoms, or unexplained hematuria, and should pursue cystoscopy when symptoms persist despite standard management [1,2].
Intravesical erosion of promontofixation mesh is an uncommon late complication that may manifest with bladder stone formation and persistent irritative lower urinary tract symptoms. Although ultrasonography can detect an intravesical calculus, it does not establish the underlying etiology; cystoscopy remains essential to confirm mesh exposure, assess the site and extent of erosion, and plan appropriate treatment. Optimal management should address both the stone and the causative foreign body, because removal of the calculus alone may lead to recurrence if intravesical mesh persists. Accordingly, definitive treatment requires complete stone clearance combined with excision or ablation of the exposed intravesical mesh to achieve symptom resolution and reduce the risk of recurrent infection and stone reformation [1,2,5].
Declarations
Ethics approval and consent to participate: Written informed consent was obtained from the patient for the publication of this case report.
Consent for publication: Written informed consent for publication of the clinical details and images was obtained from the patient.
Declaration of interests: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
- Shenhar C, Goldman HB. Management of sacrocolpopexy mesh complications—a narrative review and clinical experience from a large-volume center. Int Urogynecol J. 2025;36(2):231–41. Available from: https://doi.org/10.1007/s00192-024-05955-5
- Ward K, Bautrant E, Khatri G, Love-Jones S, Glanc P, Korte C, et al. Diagnosis and treatment of abdominally inserted (sacrocolpopexy/sacrohysteropexy) mesh complications for vault/uterine prolapse. Continence. 2024;12:101718. Available from: https://doi.org/10.1016/j.cont.2024.101718
- Begley JS, Kupferman SP, Kuznetsov DD, Kobashi KC, Govier FE, McGonigle KF, et al. Incidence and management of abdominal sacrocolpopexy mesh erosions. Am J Obstet Gynecol. 2005;192(6):1956–62. Available from: https://doi.org/10.1016/j.ajog.2005.02.062
- Nassif J, Yadav GS, Orejuela FJ, Turrentine MA. Rate of mesh erosion after sacrocolpopexy with concurrent supracervical compared with total hysterectomy: a systematic review and meta-analysis. Obstetrics & Gynecology. 2022;140(3):412–20. Available from: https://doi.org/10.1097/aog.0000000000004901
- Sobota R, Thomas D, Demetres M, Cadestin V, Mao T, Asfaw T, et al. The management and efficacy of surgical techniques used for erosive mesh in the urethra and bladder: a systematic review. Urology. 2019;134:2–23. Available from: https://doi.org/10.1016/j.urology.2019.08.001