
More Information
Submitted: February 26, 2026 | Accepted: March 04, 2026 | Published: March 05, 2026
Citation: Elafari MA, Ayoub M, Bibat MA, Anas R, Youssef M, Slaoui A, et al. Febrile Lumbar Pain Revealing a Massive Collection: Complicated Psoas Abscess Managed Surgically. J Clin Med Exp Images. 2026; 10(1): 010-012. Available from:
https://dx.doi.org/10.29328/journal.jcmei.1001041.
DOI: 10.29328/journal.jcmei.1001041
Copyright license: © 2026 Elafari MA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Promontofixation; Mesh erosion; Intravesical erosion; Bladder calculus; Cystoscopy

Febrile Lumbar Pain Revealing a Massive Collection: Complicated Psoas Abscess Managed Surgically
Mohammed Amine Elafari* , Mamad Ayoub, Mohammed Amine Bibat, Rhayour Anas, Maachi Youssef, Amine Slaoui, Tarik Karmouni, Abdelatif Koutani and Khalid Elkhader
, Mamad Ayoub, Mohammed Amine Bibat, Rhayour Anas, Maachi Youssef, Amine Slaoui, Tarik Karmouni, Abdelatif Koutani and Khalid Elkhader
Urology B Department, Ibn Sina Hospital, University Hospital Center IBN SINA, University Mohammed V, Rabat, Morocco
*Corresponding author: Mohammed Amine Elafari, Urology B Department, Ibn Sina Hospital, University Hospital Center IBN SINA, University Mohammed V, Rabat, Morocco, Email: [email protected]
Psoas abscess is a rare but potentially life-threatening condition with non-specific clinical manifestations. The condition may be primary or secondary, depending on whether it has an underlying cause. The condition may be diagnosed with the help of imaging studies, especially contrast-enhanced computed tomography (CT).
A 55-year-old female patient with a history of treated hypertension presented with a 15-day history of fever and left-sided low back pain. Her laboratory parameters showed a high leukocyte count of 22,000 cells/mm³ and elevated levels of C-reactive protein (367 mg/L). Her renal functions were within normal limits, and the urine culture was negative. Contrast-enhanced CT revealed a large left-sided intra-abdominal fluid collection extending from the diaphragm to the left iliac fossa, measuring 66 x 305 mm with air bubbles. The collection also showed a left-sided intramuscular psoas collection of 66 x 50 x 131 mm. The patient received intravenous broad-spectrum antibiotics (third-generation cephalosporin, aminoglycoside, and metronidazole). The patient underwent mini-lumbotomy, and nearly 1 liter of pus was drained. The patient’s postoperative course was satisfactory with complete resolution of symptoms. The histopathological examination showed non-specific changes.
Psoas abscess should be suspected in patients with febrile low back pain and inflammatory syndrome. Contrast-enhanced CT scans are essential for diagnosis and assessment of the extent of disease. In complicated cases with large abscess formation, early surgical drainage along with appropriate antibiotics will provide the best outcome.
This case highlights the importance of early diagnosis and adapted management for successfully navigating the complexities associated with this condition.
First reported by Mynter in 1881, the psoas abscess is a rare entity that usually occurs as a result of the spread of infection from the intra- or retroperitoneal space. The pathogenesis of the primary psoas abscess is not well understood. It is a difficult diagnosis to make because of the non-specific clinical presentation, which may be absent or minimal in the early stages and includes symptoms of fever, lower back pain, and psoriatic arthritis. Recent advances in modern imaging techniques, such as ultrasound and computed tomography scanning, have significantly improved the ability to diagnose, localize, and evaluate the extent of the abscess. Surgery is the gold standard for patients in whom percutaneous drainage is unsuccessful.
We present the case of a 55-year-old woman with a past medical history of hypertension treated with antihypertensive drugs who was admitted to our hospital with a 15-day history of left febrile low back pain. Laboratory studies showed leukocytosis of 22,000/mm3 and elevated C-reactive protein of 367 mg/L. Renal function was normal, and the rest of the laboratory studies did not show any abnormalities. Urinalysis and urine culture (ECBU) were negative.
Physical examination showed tenderness and guarding over the left lumbar region with fullness. The patient did not have any associated signs of urinary or gastrointestinal disease.
Computed tomography of the abdomen and pelvis with contrast showed evidence of a large intra-abdominal collection lateralized to the left side with an enhancing wall after the injection of contrast and the presence of air bubbles. This intra-abdominal collection was extending from the diaphragm to the left iliac fossa and becoming anterior in the pelvic region, measuring 66 × 305 mm. In addition to this, another well-defined intramuscular collection in the left psoas muscle was evident, along with an enhancing wall and a size of 66 × 50 × 131 mm, indicating the presence of a secondary psoas abscess (Figure 1).
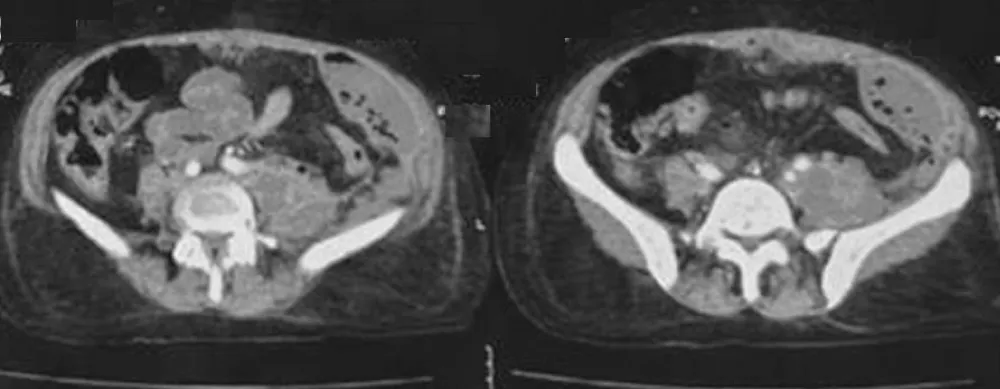
Figure 1: CT scan shows an extensive Left-Sided Intra-Abdominal Collection Extending from Diaphragm to Left Iliac Fossa with Secondary Left Psoas Abscess.
These imaging results indicated the presence of a complicated left-sided psoas abscess along with the presence of a large intra-abdominal abscess. This indicated the need for surgical intervention.
The patient was started on broad-spectrum intravenous antibiotics that included a third-generation cephalosporin, an aminoglycoside, and metronidazole. Surgical drainage was done through a mini-lumbotomy (Figure 2-A), draining almost 1 liter of pus (Figure 2-B). Biopsies of the abscess wall were sent for both bacteriological culture and histopathological analysis. Delbet drains were placed for drainage and were removed on postoperative day 7 once the drainage stopped (Figure 2-C).
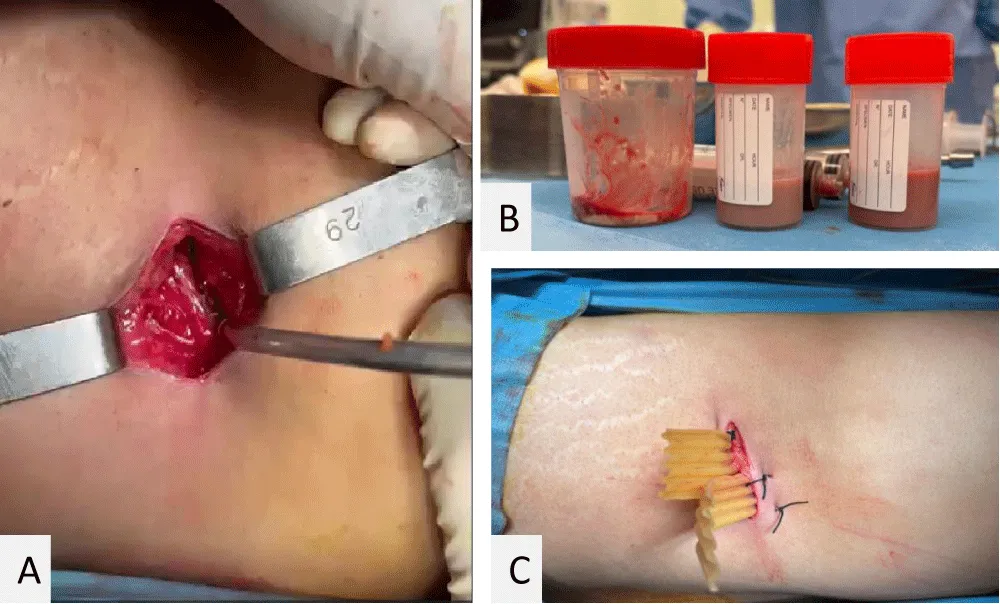
Figure 2: ER drainage of left psoas abscess: (A) mini-lumbotomy; (B) ~1 L pus; (C) Delbet drains.
The patient was discharged on postoperative day 8 on a 15-day course of oral antibiotics. At a 1-month follow-up, the patient showed excellent clinical improvement and complete resolution of the abscess on radiographs. Histopathological analysis of the abscess wall showed nonspecific inflammation, confirming the lack of malignancy or specific infectious pathology.
Psoas abscesses are generally classified into primary and secondary abscesses [1,2]. Primary abscesses, which cannot be attributed to any cause, are more prevalent in tropical countries but are a rarity in temperate countries [1]. Staphylococcus aureus is the causative agent in 90% of primary abscesses [3]. Although the exact mechanism of development is not known, some theories propose that the abscess could develop due to contamination from adenitis, hematogenous spread, or superinfection of a hematoma [2,4].
Secondary psoas abscesses, which are more prevalent in developed nations, are generally linked to an infection [5]. In Western literature, the most common cause of secondary psoas abscesses is Crohn’s disease, accounting for 54% of cases [5]. Other gastrointestinal pathologies such as appendicitis, diverticulitis, and colon cancer have also been recognized as causes [6]. Spondylodiscitis, sacroiliac arthritis, and hip arthritis, which are infectious in nature, account for 8% of cases [6]. Kidney pathologies such as kidney abscesses and pyonephrosis are rare causes [7].
Identification of predisposing factors of psoas abscess is an essential step in the risk assessment. Immunocompromised states, diabetes, and spinal interventions are significant predisposing factors [8].
Clinical manifestations of psoas abscess are non-specific. Fever, back pain, and symptoms of psoitis are common, whereas the presence of a painful mass in the flank or iliac fossa is seen in about 54% of patients [2,9].
Imaging modality improvements have greatly enhanced the sensitivity of diagnosis. Ultrasound has a sensitivity of about 80% in diagnosing psoas abscesses and can also be used to determine the underlying cause, especially in cases of renal origin [9]. Computed tomography (CT) scans have a reported sensitivity of nearly 100% for diagnosis. CT scans give a more accurate assessment of the abscess size and can also identify any associated or underlying lesions [10]. Magnetic resonance imaging (MRI) has a comparable level of sensitivity to CT scans [11].
The anatomical position of the psoas muscle contributes to the difficulties in the diagnosis of primary psoas abscess in children [2]. In patients with psoas abscess who present with febrile limp and psoitis, the diagnosis can be narrowed down to pyelonephritis, acute appendicitis, groin phlegmon, psoas abscess, and septic arthritis of the hip [4]. The typical triad of abdominal or lumbar pain, psoas, and tenderness in the iliac fossa can be used to support the diagnosis [2]. The preservation of internal and external rotation of the hip joint helps to rule out septic arthritis of the hip [2].
Ultrasound helps establish the size and location of the abscess, as well as exclude differential diagnoses [9]. Laboratory and microbiological investigations confirm the infective nature of the condition and help in monitoring the progression of the condition [3].
Currently, the treatment of primary psoas abscess is based on percutaneous drainage and antistaphylococcal antibiotic therapy. The success rate of percutaneous drainage varies from 83% to 100% [10,11].
The ultrasound features of psoas abscess formation occur in three stages, designated stages I, II, and III. During the initial stage, the psoas muscle appears to be enlarged and hypoechoic. During the collection stage, an oval hypoechoic mass with irregular edges is seen on imaging [9]. These stages, stages I and II, support non-surgical management [9].
In cases where surgical drainage is necessary, an extraperitoneal approach is used [11]. The gradual onset, delay in diagnosis ranging from 15 days to 6 months, and progressive nature of this disease may limit the effectiveness of conservative therapy [2]. Although conservative therapy, such as minimally invasive therapy and antibiotic and percutaneous drainage, is often attempted, this may be associated with recurrence and complications such as bacteremia, fistula formation, and failure to drain, especially in multiloculated abscesses [10,11].
Therefore, several authors recommend surgical drainage, either by lumbotomy or an extraperitoneal anterolateral approach to the iliac fossa, as the best treatment for selected cases [10,11].
In cases of secondary psoas abscess, definitive management must also include treatment of the underlying causative condition in a subsequent stage [5].
In conclusion, primary psoas abscesses seem to be more commonly encountered in our practice, especially in young males. The delay in presentation and diagnosis in our environment makes the success of medical and percutaneous drainage questionable. Surgical drainage remains our method of choice in this situation.
Declarations
Ethics approval and consent to participate: Written informed consent was obtained from the patient for the publication of this case report.
Consent for publication: Written informed consent for publication of the clinical details and images was obtained from the patient.
Declaration of interests: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
- Ricci MA, Rose FB, Meyer KK. Pyogenic psoas abscess: worldwide variations in etiology. World J Surg. 1986;10(5):834-843. Available from: https://dx.doi.org/10.1007/BF01655254
- Mallick IH, Thoufeeq MH, Rajendran TP. Iliopsoas abscesses. Postgrad Med J. 2004;80(946):459-462. Available from: https://dx.doi.org/10.1136/pgmj.2003.017665
- Santaella RO, Fishman EK, Lipsett PA. Primary vs secondary iliopsoas abscess. Presentation, microbiology, and treatment. Arch Surg. 1995;130(12):1309-1313. Available from: https://dx.doi.org/10.1001/archsurg.1995.01430120053008
- Navarro López V, Ramos JM, Meseguer V, et al. Microbiology and outcome of iliopsoas abscess in 124 patients. Medicine (Baltimore). 2009;88(2):120-130. Available from: https://dx.doi.org/10.1097/MD.0b013e31819d2748
- Cantasdemir M, Kara B, Cebi D, et al. Computed tomography-guided percutaneous catheter drainage of primary and secondary iliopsoas abscesses. Clin Radiol. 2003;58(10):811-815. Available from: https://dx.doi.org/10.1016/S0009-9260(03)00206-7
- Zissin R, Gayer G, Kots E, et al. Iliopsoas abscess: a report of 24 patients diagnosed by CT. Abdom Imaging. 2001;26(5):533-539. Available from: https://dx.doi.org/10.1007/s002610000214
- Gruenwald I, Abrahamson J, Cohen O. Psoas abscess: case report and review of the literature. J Urol. 1992;147(6):1624-1626. Available from: https://dx.doi.org/10.1016/S0022-5347(17)37506-1
- Almana O, Ben Yahia K, Aldhabab A, et al. (December 11, 2023) Pyogenic Psoas Abscess in a Patient With Chronic Low Back Pain: A Case Report. Cureus 15(12): e50330. Available from: https://dx.doi.org/10.7759/cureus.50330
- Lin MF, Lau YJ, Hu BS, Shi ZY, Lin YH. Pyogenic psoas abscess: analysis of 27 cases. J Microbiol Immunol Infect. 1999;32(4):261-268.Available from: https://pubmed.ncbi.nlm.nih.gov/10650491/
- Tabrizian P, Nguyen SQ, Greenstein A, Rajhbeharrysingh U, Divino CM. Management and treatment of iliopsoas abscess. Arch Surg. 2009;144(10):946-949. Available from: https://dx.doi.org/10.1001/archsurg.2009.144
- Shields D, Robinson P, Crowley TP. Iliopsoas abscess—a review and update on the literature. Int J Surg. 2012;10(9):466-469. Available from: https://dx.doi.org/10.1016/j.ijsu.2012.08.016