
More Information
Submitted: February 27, 2026 | Accepted: March 13, 2026 | Published: March 16, 2026
Citation: Elafari MA, Ayoub M, Bibat MA, Youssef M, Slaoui A, Karmouni T, et al. Bilateral Severe Encrustation of Long-Term Indwelling Double-J Stents in a Young Non-Lithiasic Patient. J Clin Med Exp Images. 2026; 10(1): 013-015. Available from:
https://dx.doi.org/10.29328/journal.jcmei.1001042.
DOI: 10.29328/journal.jcmei.1001042
Copyright license: © 2026 Elafari MA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Double-J stent; Ureteral stent; Encrustation; Staghorn calculi; Vesicovaginal Fistula; Lithiasis; Holmium Laser; Lithotripsy; Flexible Ureteroscopy; Hydronephrosis

Bilateral Severe Encrustation of Long-Term Indwelling Double-J Stents in a Young Non-Lithiasic Patient
Mohammed Amine Elafari* , Mamad Ayoub, Mohammed Amine Bibat, Maachi Youssef, Amine Slaoui, Tarik Karmouni, Abdelatif Koutani and Khalid Elkhader
, Mamad Ayoub, Mohammed Amine Bibat, Maachi Youssef, Amine Slaoui, Tarik Karmouni, Abdelatif Koutani and Khalid Elkhader
Urology B Department, Ibn Sina Hospital, University Hospital Center IBN SINA, University Mohammed V, Rabat, Morocco
*Corresponding author: Mohammed Amine Elafari, Urology B Department, Ibn Sina Hospital, University Hospital Center IBN SINA, University Mohammed V, Rabat, Morocco, Email: [email protected]
Ureteral double-J stents are a commonly used device in urological practice to allow urinary drainage, avoid ureteral obstruction processes, and protect the upper urinary tract after surgical procedures. However, long indwelling time may give rise to numerous complications, such as infection, migration, and fragmentation of the stent, especially encrustation. Encrustation of stents is a well-known complication that has been closely related to the time active of the stent and can cause significant morbidity if not timely addressed. In severe cases, abundant mineral deposition can result in the development of large calculi encasing the stent and rarely progress to staghorn stones. These cases may pose challenges in terms of the extraction of the stent and may result in complex endourological intervention. The encrustation likelihood is substantially higher if stents are left forgotten or remain in place longer than the advised period. Most patients with heavily encrusted stents have symptoms including flank pain, urinary tract infection, hematuria, or obstructive uropathy, but can present without any symptoms, and this can delay the diagnosis.
We present the case of a 25-year-old female patient who underwent the insertion of bilateral JJ ureteral stents as part of the surgical management of a vesicovaginal fistula secondary to an obstetric complication. The patient was found to have severe proximal encrustations of the stents with heterogeneous staghorn calculi encasing both proximal stent coils on follow-up. Contrast-enhanced computed tomography was used to assess the extent of encrustation. The patient was treated successfully with flexible ureteroscopy using holmium laser lithotripsy for the fragmentation of the encrustations. Normal renal function was observed in the patient. The urine was sterile. The case emphasizes the importance of strict stent-tracking protocols to avoid the occurrence of this preventable complication in patients with indwelling JJ ureteral stents.
A 25-year-old woman with no prior history of urolithiasis underwent bilateral double-J (JJ) ureteral stent placement as part of surgical repair of a vesicovaginal fistula due to obstetric trauma secondary to cesarean delivery. The stents were left in place postoperatively for 6 months without removal.
The patient was referred for evaluation. Clinically, she did not have flank pain, fever, hematuria, or other urinary symptoms.
The laboratory studies showed normal renal function with a serum creatinine of 0.8 mg/dL and blood urea nitrogen of 24 mg/dL. Other inflammatory markers were all within normal limits, with a white blood cell count of 6.2 ×10⁹/L and C-reactive protein < 3 mg/L.
Serum electrolytes, including calcium 9.4 mg/dL, phosphate 3.5 mg/dL, and uric acid 4.2 mg/dL, were normal. Urinalysis did not demonstrate leukocyturia or hematuria, and the urine culture was sterile.
A urolithiasis metabolic evaluation was also conducted. 24-hour urine analysis showed a urinary volume of 2.1 L/24 h, calcium at 180 mg/24 h, oxalate at 32 mg/24 h, citrate at 520 mg/24 h, uric acid at 520 mg /24 h, and sodium at 130 mmol/24 h.
These findings did not identify any metabolic abnormality predisposing to stone formation.
Contrast-enhanced computed tomography showed bilateral proximal stent encrustations. On the right side, a heterogeneous staghorn calculus measuring 28 × 23 × 16 mm (601 HU) partially enveloped the proximal coil of the stent, causing moderate tricalyceal dilatation with maintained cortical thickness. Three additional non-obstructive inferior calyceal stones were also present. On the left side, a heterogeneous staghorn calculus measuring 28 × 17 × 25.5 mm (486 HU) surrounded the proximal coil of the stent with moderate upstream dilatation. No ureteral stones were identified (Figure 1A,B).
Endoscopic treatment was undertaken using flexible ureteroscopy and holmium laser lithotripsy with good fragmentation and removal of the encrustations (Figure 1C,D).
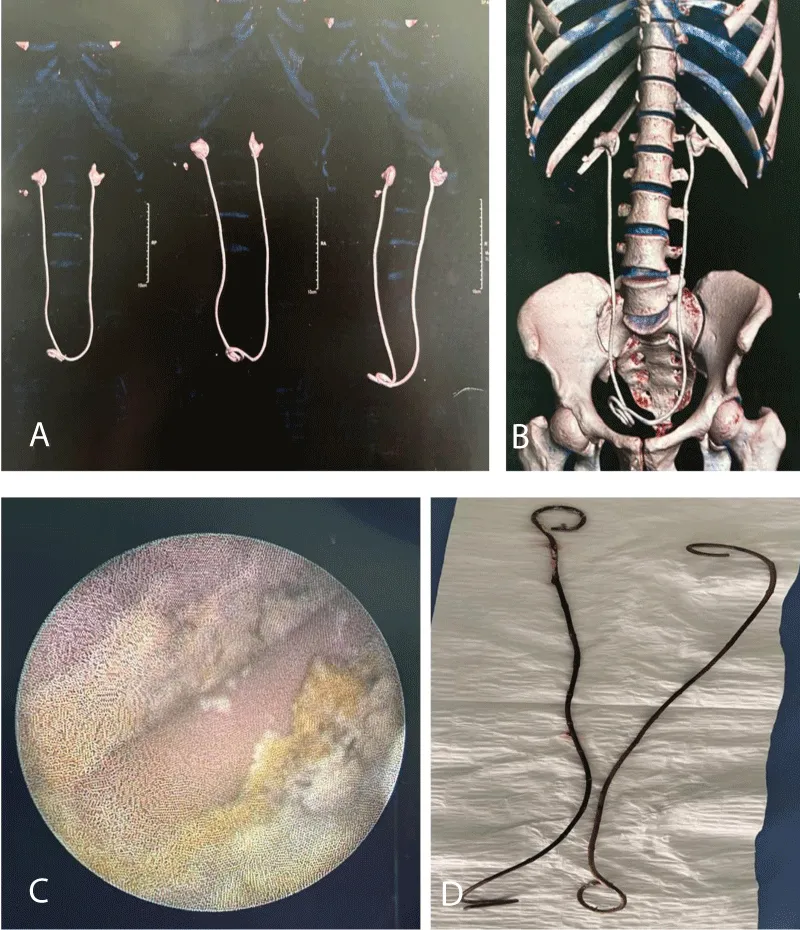
Figure 1: A. Severe bilateral proximal encrustation of long-term indwelling double-J ureteral stents with staghorn calculus formation. B. CT imaging and 3D reconstruction demonstrate bilateral stone burden with hydronephrosis. C. Endoscopic view shows calcified encrustation of the proximal coil. D. Extracted stents after holmium laser lithotripsy reveal extensive proximal mineralization.
Diagnosis
Severe bilateral proximal encrustation of long-term indwelling double-J ureteral stents with associated staghorn calculus formation and secondary hydronephrosis [1,2].
Double-J stenting of the ureter is a common practice in the field of urology for temporary diversion and post-operative stenting. Encrustation of stents is a known complication and is heavily correlated with the duration of stenting. The rate of encrustation is increased after 6–12 weeks of stenting and is particularly high after several months.
While encrustation is more often linked to lithiasic disease or urinary tract infection, it can also occur in non-lithiasic patients. The pathophysiological process involves the development of a biofilm and subsequent progressive mineralization of the stent surface, which can potentially act as a nidus for stone formation [3]. Retained stents for a long period of time can result in the development of complex calculi, obstruction, hydronephrosis, infection, and potentially irreversible renal injury if left untreated [4].
The FECal system of classification is a useful tool for assessing the severity of stent encrustation and determining treatment [5]. Treatment in these patients may require sophisticated endourological interventions, such as ureteroscopy with laser lithotripsy or a combination of percutaneous procedures in more severe cases [4].
This particular case illustrates that severe encrustation of bilateral stents can also occur in young non-lithiasic patients if the stents are retained for a long period of time. It is important to establish a stent-tracking system to prevent this potentially serious complication.
Declarations
Ethics approval and consent to participate: Written informed consent was obtained from the patient for the publication of this case report.
Consent for publication: Written informed consent for publication of the clinical details and images was obtained from the patient.
Declaration of interests: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
- El-Faqih SR, Shamsuddin AB, Chakrabarti A, Atassi R, Kardar AH, Osman MK, et al. Polyurethane internal ureteral stents in the treatment of stone patients: morbidity related to indwelling times. J Urol. 1991;146:1487– 1491. Available from: https://doi.org/10.1016/s0022-5347(17)38146-6
- Kawahara T, Ito H, Terao H, Yoshida M, Matsuzaki J. Ureteral stent encrustation, incrustation, and coloring: morbidity related to indwelling times. J Endourol. 2012;26:178–182. Available from: https://doi.org/10.1089/end.2011.0385
- Lam JS, Gupta M. Tips and tricks for the management of retained ureteral stents. J Endourol. 2002;16:733–741. Available from: https://doi.org/10.1089/08927790260472881
- Bultitude MF, Tiptaft RC, Glass JM, Dasgupta P. Management of encrusted ureteral stents impacted in the upper tract. Urology. 2003;62:622–626. Available from: https://doi.org/10.1016/s0090-4295(03)00506-5
- Acosta-Miranda AM, Milner J, Turk TM. The FECal Double-J classification: a simplified approach in the management of encrusted and retained ureteral stents. J Endourol. 2009;23:409–415. Available from: https://doi.org/10.1089/end.2008.0214