
More Information
Submitted: March 22, 2026 | Accepted: March 28, 2026 | Published: March 30, 2026
Citation: Elafari MA, Ayoub M, Bibat MA, Slaoui A, Karmouni T, Koutani A, et al. Not Every Bladder Mass Is Malignant: A Case of Inverted Urothelial Papilloma in a Young Adult. J Clin Med Exp Images. 2026; 10(1): 016-019. Available from:
https://dx.doi.org/10.29328/journal.jcmei.1001043.
DOI: 10.29328/journal.jcmei.1001043
Copyright license: © 2026 Elafari MA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Inverted urothelial papilloma; Bladder tumor; Differential diagnosis; Immunohistochemistry; Young adult

Not Every Bladder Mass Is Malignant: A Case of Inverted Urothelial Papilloma in a Young Adult
Mohammed Amine Elafari* , Mamad Ayoub, Mohammed Amine Bibat, Amine Slaoui, Tarik Karmouni, Abdelatif Koutani and Khalid Elkhader
, Mamad Ayoub, Mohammed Amine Bibat, Amine Slaoui, Tarik Karmouni, Abdelatif Koutani and Khalid Elkhader
Urology B Department, Ibn Sina Hospital, University Hospital Center IBN SINA, University Mohammed V, Rabat, Morocco
*Corresponding author: Mohammed Amine Elafari, Urology B Department, Ibn Sina Hospital, University Hospital Center IBN SINA, University Mohammed V, Rabat, Morocco, Email: [email protected]
Inverted Urothelial Papilloma (IUP) is an unusual variety of urothelial tumors that typically occurs in adults, with a predominance in males. The definitive diagnosis of IUP relies on histopathological examination, as the clinical presentation and endoscopic appearance are non-specific. The recommended treatment for IUP includes the complete transurethral resection, with some controversy regarding the need for cystoscopic follow-up. In this case, we present an atypical instance of IUP in a 21-year-old male patient, diagnosed with gross hematuria and irritative lower urinary tract symptoms. A clinical assessment revealed a 3.0 × 2.6 cm intravesical mass. The definitive diagnosis was confirmed histopathologically and further substantiated by immunohistochemistry, which demonstrated low expression of p53 and Ki-67, effectively ruling out malignancy. This case underscores the diagnostic challenges posed by bladder masses in young adults, emphasizing the necessity of integrating morphological and immunohistochemical findings to prevent overdiagnosis of urothelial carcinoma. The paper focuses on the diagnostic approach and management of this rare condition in the young male population.
Inverted urothelial papilloma (IUP) is an uncommon benign urothelial tumor with an endophytic growth pattern. IUP accounts for 1% - 2% of all urothelial tumors, predominantly occurs in men between the ages of 50 and 60 years, with a male-to-female ratio of 6:1. The most common location of IUP is the bladder trigone, followed by the bladder neck, though it may occur anywhere in the urinary tract [1-3].
The classic presentation of IUP is gross hematuria, often with irritative lower urinary tract symptoms, though the cytology is invariably negative [1,3]. In cystoscopy, IUP is a smooth surfaced, non-papillary polypoid lesion, which cannot be differentiated from other bladder tumors [1,3].
Although this tumor has traditionally been regarded as benign, it poses problems in terms of differential diagnosis because of its morphologic similarities with endophytic urothelial carcinoma [1].
Recent molecular investigations have confirmed the benign nature of IUP, showing activating mutations in genes belonging to the RAS gene family (HRAS, KRAS, NRAS), but lacking mutations associated with urothelial carcinoma (FGFR3, TP53, TERT promoter) [4-6]. The relationship between IUP and urothelial carcinoma is still debated, with reported rates of synchronous or metachronous carcinoma varying from 1.15% to 4.2% [2].
The occurrence of Inverted Urothelial Papilloma (IUP) in a 21-year-old patient is particularly unusual, as this condition typically manifests in the fifth or sixth decade of life. This case is noteworthy for its rarity and the potential for its publication to raise awareness of benign differential diagnoses in this younger demographic.
The patient, a current smoker with a 2-pack-year history, presented after one month of persistent symptoms, including gross hematuria associated with irritative lower urinary tract symptoms. The patient exhibited no substantial urological, familial, or occupational history associated with bladder carcinogens.
The initial assessment revealed that the patient was afebrile, hemodynamically stable, and in good general condition. A physical examination was conducted, which included an abdominal palpation. The results of this examination were unremarkable. Given the presence of irritative symptoms, a digital rectal examination was performed to rule out associated prostatitis or prostatic abnormalities, though it remained unremarkable.
Abdominal ultrasound revealed a well-defined sessile, non-mobile, and mildly vascularized echogenic intravesical mass arising from the left lateral bladder wall (Figure 1).
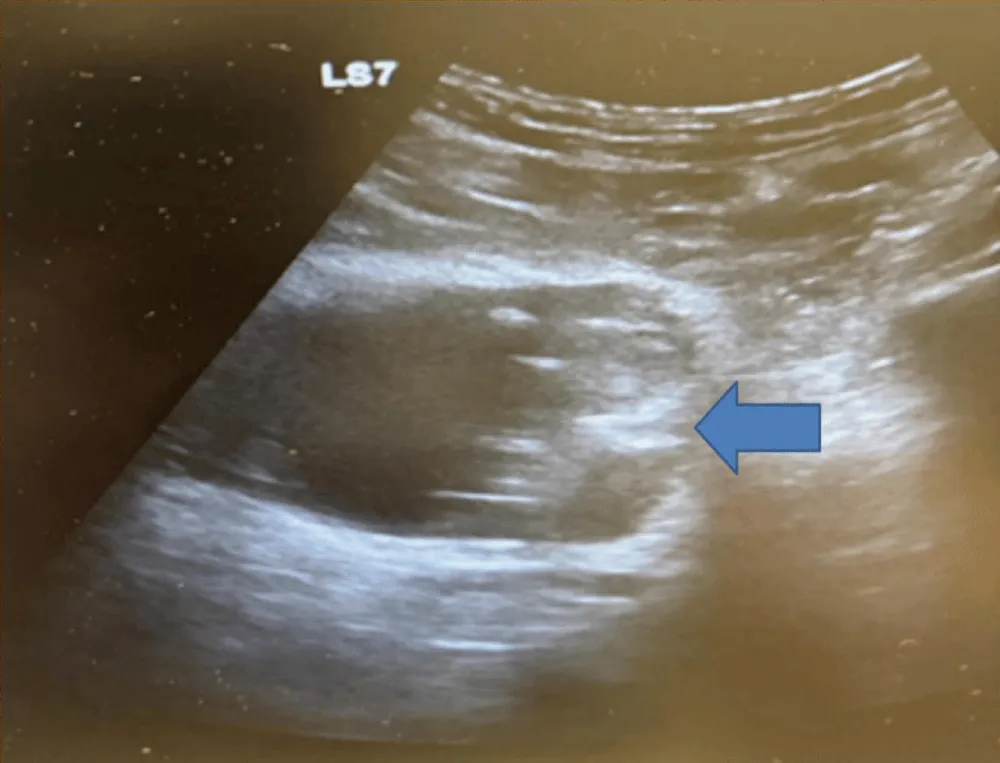
Figure 1: Radiological Assessement. Abdominal ultrasound showing a well-defined sessile, non-mobile, and mildly vascularized echogenic intravesical mass arising from the left lateral bladder wall.
Subsequent contrast-enhanced CT, performed during portal and excretory phases, confirmed a well-circumscribed soft tissue mass measuring 3.0 × 2.6 cm with homogenous enhancement and no signs of perivesical fat invasion. The lesion was located on the left lateral wall, distinct from the ureteral orifice and the bladder neck, explaining the absence of upper tract dilatation (Figure 2).
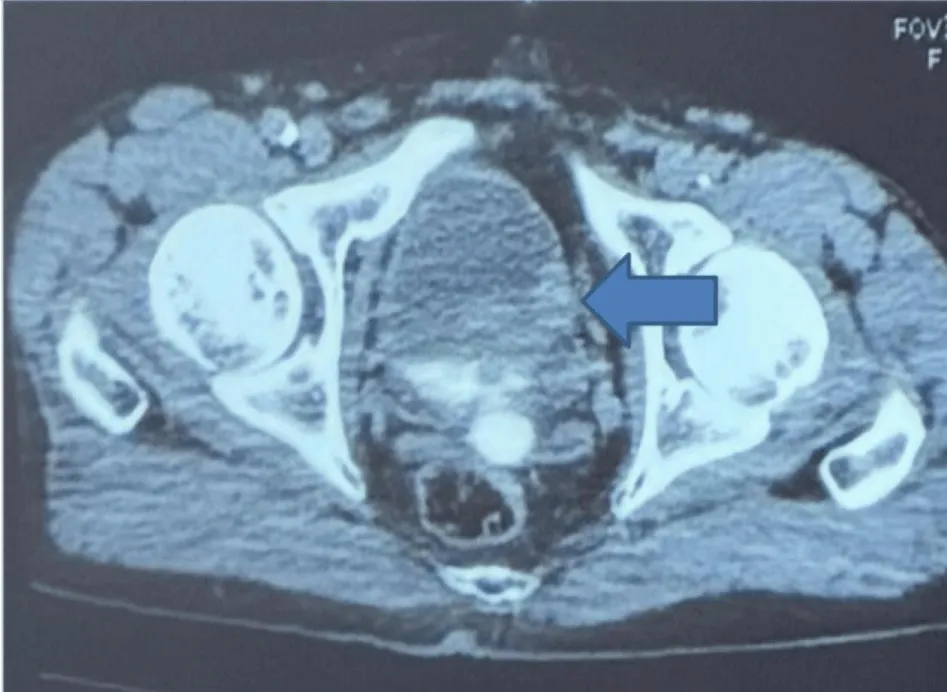
Figure 2: Computed Tomography Findings. Axial contrast-enhanced CT scan confirming a well-circumscribed intravesical soft tissue mass measuring 3.0 × 2.6 cm with homogenous enhancement and no signs of perivesical fat Invasion. The lesion was located on the left lateral wall, distinct from the ureteral orifice and the bladder neck, explaining the absence of upper tract dilatation.
Preoperative laboratory investigations, including serum creatinine and complete blood count, were within normal limits. Urinalysis and urine culture were negative, and urinary cytology showed no evidence of malignancy.
Cystoscopy demonstrated a non-papillary polypoid lesion with a smooth surface, approximately 3 cm in size, located in the left lateral wall (Figure 3).
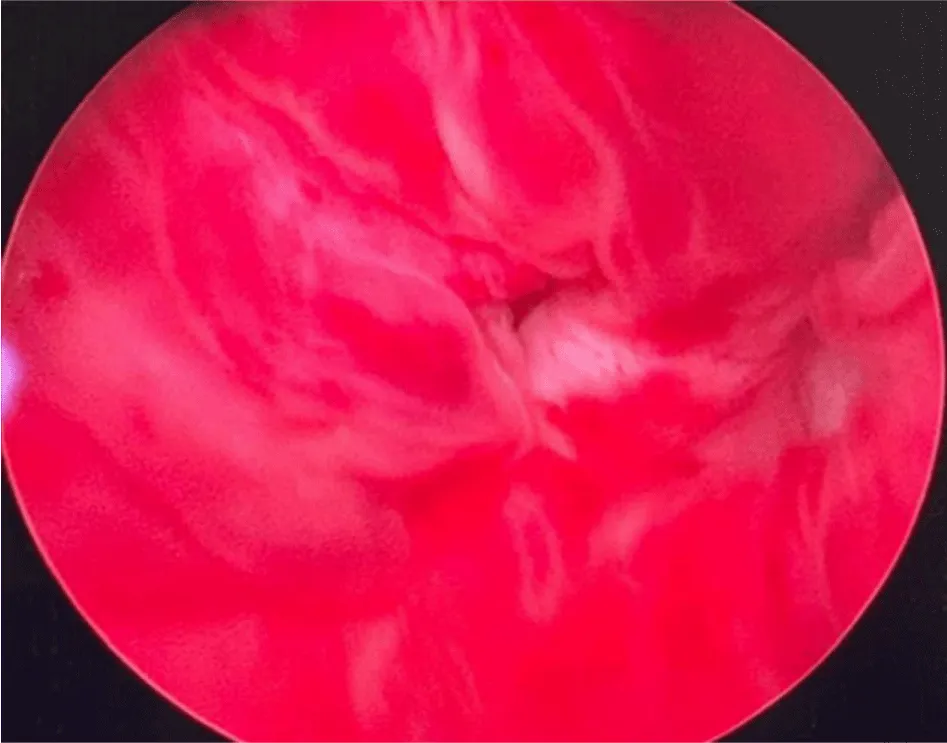
Figure 3: Endoscopic Appearance. Cystoscopic image showing a non-papillary polypoid sessile lesion with a smooth surface, approximately 3 cm in size, located in the left lateral bladder wall.
Following the complete transurethral resection of the bladder lesion, histopathological examination revealed an endophytic urothelial proliferation with an inverted growth pattern, characterized by cytologically bland cells with minimal atypia and low mitotic activity. Immunohistochemical staining demonstrated low expression of p53 and Ki-67, consistent with a benign process and supporting the diagnosis of inverted urothelial papilloma (Figure 4).
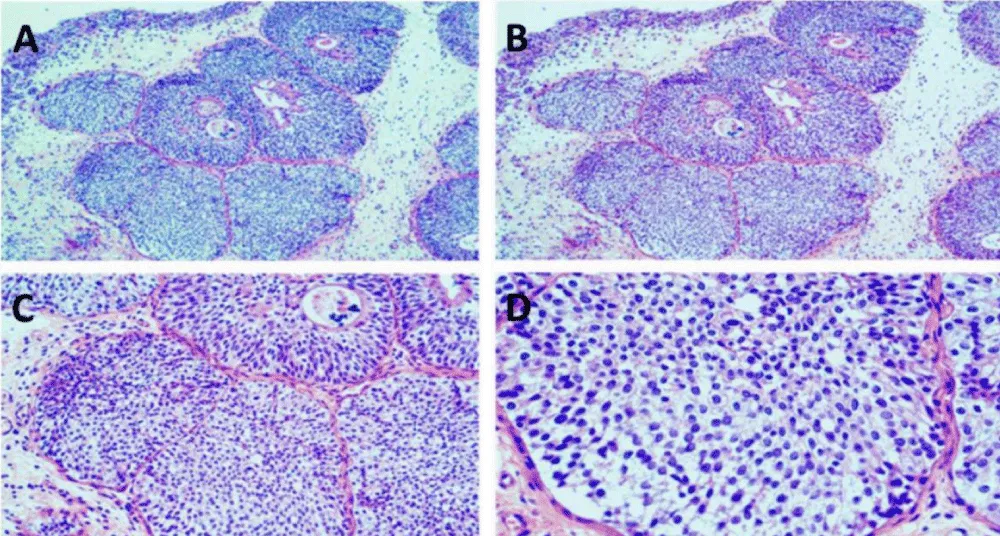
Figure 4: Histopathological and Immunohistochemical Analysis. A-D: Pathological features of Inverted Urothelial Papilloma (Hematoxylin and Eosin and Immunohistochemistry). A. (Low power, x40): Structural organization of urothelial nests showing an endophytic growth pattern. B. (Intermediate power x 100): Nested architecture with cytologically bland urothelial cells. C. (View x 200): Presence of microcystic spaces and areas of glandular differentiation. D. (High power view x 400): Monomorphic cells with minimal atypia and low mitotic activity, consistent with a benign process.
Follow-up cystoscopy at 3 and 6 months showed no evidence of recurrence.
Informed consent was obtained from the patient for the surgical procedure and for the publication of this case report, including the associated clinical and radiological images, while ensuring total anonymity.
This case is also significant due to the occurrence of IUP in a 21-year-old patient, which is rare considering that this condition usually occurs in the fifth or sixth decade of life [1,3]. The gross hematuria and irritative lower urinary tract symptoms presented by the patient are consistent with the typical presentation of IUP [1,3].
The primary diagnostic challenge lies in differentiating IUP from low-grade urothelial carcinoma with an inverted growth pattern, as these two conditions can manifest similarly [1].
Histopathological evaluation with strict adherence to established criteria is essential in the definitive diagnosis of IUP. These criteria include an endophytic growth pattern, cytologically bland urothelial cells, minimal atypia, low mitotic activity, and frequent microcystic changes [1]. As seen in our case (Figure 4), the lesion exhibited a nested architecture with monomorphic cells and glandular differentiation. Two architectural patterns have been recognized: trabecular (streaming) and glandular (cystic), which could be related to different RAS gene mutations [5].
Immunohistochemistry may also be helpful in difficult cases. While IUP tends to be negative or have low expression of Ki-67, p53, and cytokeratin 20 (CK20), urothelial carcinoma with inverted pattern tends to stain positively in 59% to 90% of cases [7,8]. In our case, low p53 and Ki-67 were supportive of benign behaviour (Figure 4). Fluorescence in situ hybridization (FISH) may also be helpful because IUP lacks the chromosomal alterations seen in urothelial carcinoma [7,8].
Recent studies have revealed that IUP is distinguished by activating mutations in the RAS gene family (HRAS, KRAS, NRAS), while exhibiting a lack of mutations characteristic of urothelial carcinoma, such as FGFR3 or TP53. Furthermore, the reported rates of synchronous or metachronous carcinoma (1.15% - 4.2%) must be interpreted with caution, as these figures vary significantly depending on the stringency of the histological diagnostic criteria applied and the specific characteristics of the case series analysed [1,5,6].
Complete transurethral resection is the standard treatment for IUP [1,3]. The necessity of post-resection surveillance is controversial. Early studies indicated an association between IUP and urothelial carcinoma, suggesting that intensive post-resection surveillance is necessary [2]. However, recent studies with the implementation of strict criteria for diagnosis have shown that recurrence is extremely low, leading some authors to question the necessity of post-resection surveillance [3,4,9].
Sung, et al. noted that only 1 recurrence was observed in 75 patients with a mean follow-up of 68 months, concluding that as rigorous a surveillance protocol as that recommended for urothelial carcinoma is not necessary if strict criteria are followed and complete resection is performed [3]. Patel, et al. did not note any progression in their study, concluding that continuous surveillance is not necessary if the diagnosis is correct without evidence of previous or concurrent urothelial carcinoma [4].
On the other hand, Picozzi, et al. in their systematic review of 365 patients, suggested that close cystoscopic follow-up should be performed on the basis of the association with synchronous or metachronous urothelial carcinoma [2].
A balanced approach that takes into account individual patient-related factors, including the patient’s age, smoking history, completeness of resection, and confidence in the histopathologic diagnosis, is necessary.
In the current case, the young patient underwent complete resection with a definitive histopathologic diagnosis, and the patient underwent follow-up cystoscopy at 3 and 6 months, showing no evidence of recurrence. In IUP, with a benign molecular profile and good prognosis with appropriate diagnosis, the follow-up may not need to be as rigorous as that of urothelial carcinoma [3,4,9].
Inverted urothelial papilloma (IUP) is a rare type of benign tumor of the bladder, although typically found in older man it may occur in young adults. The clinical and endoscopic findings of IUP are non-specific, and thus histopathologic examination of the tumor is mandatory for the diagnosis. The treatment of IUP involves complete transurethral resection of the tumor. Although the need for rigorous cystoscopic follow-up of patients with IUP is controversial, recent data indicate that if the diagnostic criteria are strictly applied and complete resection of the tumor is achieved, less rigorous follow-up may be recommended than that required for urothelial carcinoma. The follow-up should be tailored to the individual patient based on the level of diagnostic certainty, age, and completeness of resection. Our patient had a favorable postoperative course with no evidence of recurrence during follow-up which highlights the importance of complete resection and careful histopathological evaluation for optimal outcomes.
Declaration
Ethical approval: Ethics approval has been obtained to proceed with the current study.
Ethical approval for this study (Ethical Committee N009-24) was provided by the Ethical Committee Ibn University Hospitals, Rabat Morocco on 22 January 2024
Consent: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of the journal.
Guarantor of submission: The corresponding author is the guarantor of submission.
Availability of data and materials: Supporting material is available if further analysis is needed.
Provenance and peer review: Not commissioned, externally peer-reviewed.
- Kitahama K, Inamura K. Inverted urothelial papilloma: Diagnostic challenges, molecular insights, and clinical implications. Histol Histopathol. 2026 Mar 10:25058. Epub ahead of print. PMID: 41804641. Available from: https://doi.org/10.14670/hh-25-058
- Picozzi S, Casellato S, Bozzini G, Ratti D, Macchi A, Rubino B, et al. Inverted papilloma of the bladder: A review and an analysis of the recent literature of 365 patients. Urol Oncol. 2013;31(8):1584-90. Available from: https://doi.org/10.1016/j.urolonc.2012.03.009
- Sung MT, Maclennan GT, Lopez-Beltran A, Montironi R, Cheng L. Natural history of urothelial inverted papilloma. Cancer. 2006;107(11):2622-7. Available from: https://doi.org/10.1002/cncr.22311
- Patel P, Reikie BA, Maxwell JP, Yilmaz A, Gotto GT, Trpkov K. Long-term clinical outcome of inverted urothelial papilloma including cases with focal papillary pattern: Is continuous surveillance necessary? Urology. 2013;82(4):857-60. Available from: https://doi.org/10.1016/j.urology.2013.06.040
- Kitahama K, Shigematsu Y, Amori G, Sugawara E, Yonese J, Shibahara J, et al. RAS family gene mutations, clinicopathological features, and spread patterns of inverted urothelial papilloma of the bladder. Am J Surg Pathol. 2024;48(4):458-464. Available from: https://doi.org/10.1097/pas.0000000000002171
- Isharwal S, Hu W, Sarungbam J, Chen YB, Gopalan A, Fine SW, et al. Genomic landscape of inverted urothelial papilloma and urothelial papilloma of the bladder. J Pathol. 2019;248(3):260-265. Available from: https://doi.org/10.1002/path.5261
- Sun JJ, Wu Y, Lu YM, Zhang HZ, Wang T, Yang XQ, et al. Immunohistochemistry and fluorescence in situ hybridization can inform the differential diagnosis of low-grade noninvasive urothelial carcinoma with an inverted growth pattern and inverted urothelial papilloma. PLoS One. 2015;10(7):e0133530. Available from: https://doi.org/10.1371/journal.pone.0133530
- Jones TD, Zhang S, Lopez-Beltran A, Eble JN, Sung MT, MacLennan GT, et al. Urothelial carcinoma with an inverted growth pattern can be distinguished from inverted papilloma by fluorescence in situ hybridization, immunohistochemistry, and morphologic analysis. Am J Surg Pathol. 2007;31(12):1861-1867. Available from: https://doi.org/10.1097/pas.0b013e318060cb9d
- Liu Z, Wei S, Tang J. Clinicopathologic features of noninvasive inverted urothelial tumor. Am J Clin Oncol. 2023;46(9):409-413. Available from: https://doi.org/10.1097/coc.0000000000001027