
More Information
Submitted: March 18, 2026 | Accepted: March 31, 2026 | Published: April 01, 2026
Citation: Elafari MA, Ayoub M, Zaki MA, Bibat MA, Slaoui A, Karmouni T, et al. Adult Bladder Exstrophy with Premalignant Changes Following Failed Reconstruction: A Case Report. J Clin Med Exp Images. 2026; 10(1): 020-023. Available from:
https://dx.doi.org/10.29328/journal.jcmei.1001044.
DOI: 10.29328/journal.jcmei.1001044
Copyright license: © 2026 Elafari MA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Bladder exstrophy; Squamous metaplasia; Radical cystectomy; Ileal conduit; Vesicocutaneous fistula

Adult Bladder Exstrophy with Premalignant Changes Following Failed Reconstruction: A Case Report
Mohammed Amine Elafari* , Mamad Ayoub, Mohamed Amine Zaki, Mohammed Amine Bibat, Amine Slaoui, Tarik Karmouni, Abdelatif Koutani and Khalid Elkhader
, Mamad Ayoub, Mohamed Amine Zaki, Mohammed Amine Bibat, Amine Slaoui, Tarik Karmouni, Abdelatif Koutani and Khalid Elkhader
Urology B Department, Ibn Sina Hospital, University Hospital Center IBN SINA, University Mohammed V, Rabat, Morocco
*Corresponding author: Mohammed Amine Elafari, Urology B Department, Ibn Sina Hospital, University Hospital Center IBN SINA, University Mohammed V, Rabat, Morocco, Email: [email protected]
Background: Bladder exstrophy is a rare congenital abnormality that is usually managed with multiple surgical interventions. Long-term consequences include recurrent urinary tract infections, bladder stones, fistulae, and metaplastic changes with malignant potential.
Case Presentation: We present a case of a 21-year-old male with a history of failed childhood surgeries for bladder exstrophy who presented with a vesicocutaneous fistula and a 7 cm bladder stone. He underwent an open cystolithotomy with bladder augmentation and creation of a Benchekroun continent valve. However, the patient developed recurrent fistulae due to poor tissue quality. Histopathological examination confirmed early squamous metaplasia in the bladder mucosa. After discussion in a multidisciplinary meeting, the patient underwent a radical cystectomy with ileal conduit urinary diversion using the Bricker technique. He is doing well at 3 months with no evidence of any complication.
Conclusion: This case illustrates the difficulties encountered in managing adult patients with bladder exstrophy and failed reconstructions. The presence of squamous metaplasia, poor bladder tissue, and recurrent complications all contributed to the decision for radical cystectomy. It is important to recognize these changes and address them appropriately in a timely manner to prevent further complications and possible malignant changes.
Bladder exstrophy is a rare congenital abnormality that occurs in approximately 1 in 30,000–50,000 live births, with a predominance of males [1]. Bladder exstrophy is a spectrum of genitourinary anomalies that require complex reconstructive surgery, which is often multiple-staged during the child’s growth and development. Despite advances in surgical techniques, the long-term outcomes are still unpredictable, with varying degrees of success with urinary continence ranging from 30% to 80% depending on the surgical technique [2,3].
Bladder exstrophy patients have many long-term complications, including urinary incontinence, recurrent urinary tract infections, bladder stones, upper urinary tract damage, as well as histological changes in the bladder mucosa, including premalignant lesions such as squamous metaplasia that may lead to the development of bladder cancer [4,5]. One of the most serious is squamous metaplasia, especially the keratinizing type, which is a serious risk factor for the development of squamous cell carcinoma [6-8].
We report a case of a young adult with bladder exstrophy, multiple failed reconstructive surgeries, and the need for a radical cystectomy due to poor bladder quality, recurrent complications, and the presence of squamous metaplasia requiring definitive surgical management.
A 21-year-old male with a history of bladder exstrophy presented to our department with persistent urinary leakage and recurrent urinary tract complications. The patient exhibited a medical history marked by unsuccessful reconstructive surgical interventions, as detailed in his clinical records. These prior interventions included initial bladder closure and epispadias repair performed during early childhood at another facility. However, subsequent attempts to address persistent leakage and achieve continence resulted in extensive scarring and compromised pelvic anatomy, leading to severely devitalized tissue observed during the current management. The patient also exhibited recurrent bladder calculus, which was treated with endoscopic procedures.
The patient was found to be alert, oriented, and in good general condition. Physical examination showed a vesicocutaneous fistula with direct visualization of a bladder calculus and urinary leakage through the fistula. No other abnormalities were noted on physical examination (Figure 1).

Figure 1: Clinical photograph demonstrating vesicocutaneous fistula with a visible bladder stone. The fistulous opening in the suprapubic region allows direct visualization of the large bladder calculus with spontaneous urinary leakage through the cutaneous tract.
Laboratory investigations were found to be within normal limits. The complete blood count showed hemoglobin 14.2 g/dL, white blood cell count 7.5 × 10³/µL, and platelets 250 × 10³/µL. Renal function tests showed serum creatinine 0.9 mg/dL, blood urea nitrogen 14 mg/dL. Electrolyte studies were found to be within normal limits. Urinalysis showed hematuria (++), with negative leukocytes and nitrite.
The contrast-enhanced computed tomography scan of the abdomen and pelvis confirmed the presence of a 7 cm bladder calculus occupying the entire lumen of the bladder, with associated irregularity of the bladder wall and the persisting fistula tract. However, the absence of hydronephrosis and the normal size and shape of the kidneys indicated the functioning state of the upper urinary tract (Figure 2).
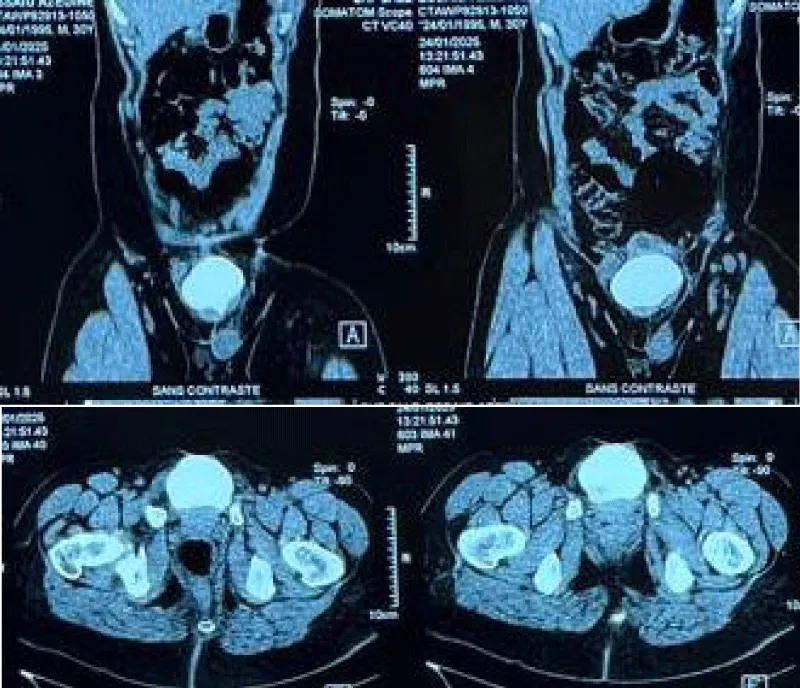
Figure 2: Contrast-enhanced computed tomography (CT) scan, axial view, demonstrating a 7 cm bladder calculus occupying the entire bladder lumen. Note the irregular bladder wall thickening and the fistulous tract extending to the anterior abdominal wall. No upper urinary tract dilation was observed.
The patient underwent open cystolithotomy, and the 7 cm bladder calculus was successfully removed. Biopsies were taken from the edges of the fistula and the bladder mucosa for histopathological examination. At the same time, the procedure of bladder augmentation through enterocystoplasty, along with the construction of a Benchekroun continent catheterizable channel, was attempted (Figures 3,4).
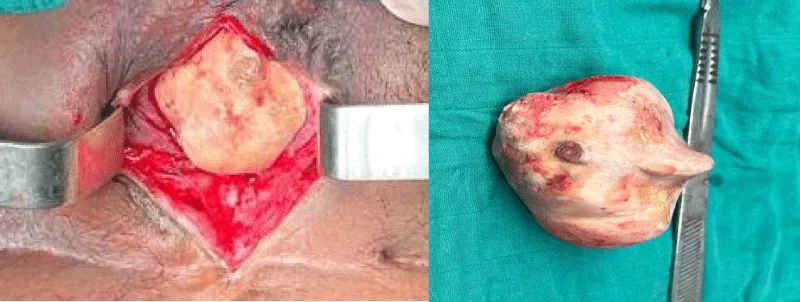
Figure 3: Intraoperative view of the extracted bladder stone measuring 7 cm.
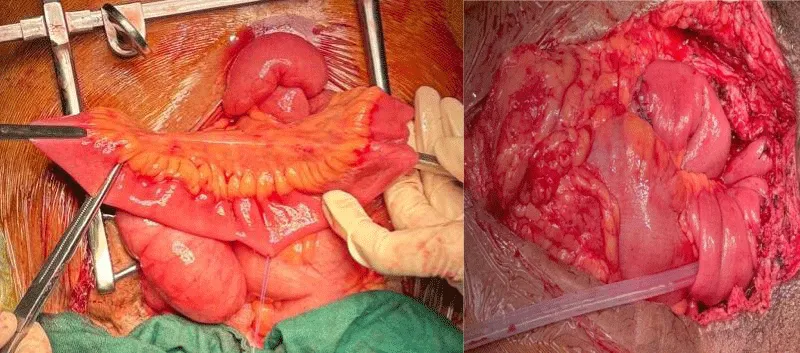
Figure 4: Detubularized bowel segment prepared for enterocystoplasty with the Benchekroun channel.
During the postoperative course, the patient again presented with the vesicocutaneous fistula, which was attributed to poor vascularization and fibrosis of the native bladder plate. The histopathology of the biopsy samples confirmed the presence of early non-keratinizing squamous metaplasia without dysplasia in the bladder mucosa, which is of grave concern as it may lead to the development of malignancy (Figure 5).

Figure 5: Recurrent vesicocutaneous fistula following failed reconstruction.
In due course, after deliberation by a multidisciplinary team consisting of urologists, pathologists, and the patient, as well as his family members, it was decided to perform a radical cystectomy with ileal conduit urinary diversion, also known as the Bricker procedure. The reasons behind this radical surgical intervention were as follows: (1) poor tissue quality with recurrent fistula formation, (2) squamous metaplasia with a potential for malignancy, (3) recurrent bladder calculus, and (4) failure of all reconstructive procedures in the past.
The patient underwent radical cystectomy with ileal conduit urinary diversion satisfactorily without any complications. The patient was found to be in excellent general condition 3 months post-operatively with no signs of recurrent fistula, urinary tract infection, etc. The patient was satisfied with the surgical outcome.
This case highlights several key points regarding the long-term management of bladder exstrophy in the adult population. Adult presentation is rare and often associated with failed or absent neonatal repair. Despite multiple attempts at surgical repair in the childhood years, this patient continued to experience complications with recurrent bladder calculus and the development of a fistula.
The presence of squamous metaplasia in the bladder mucosa is also significant in this case. Various studies have indicated that patients with bladder exstrophy exhibit increased levels of squamous metaplasia compared to normal individuals, with increased levels of this abnormality occurring in patients with delayed closure [6]. Rubenwolf, et al. reported that severe epithelial abnormalities, such as cystitis glandularis and intestinal metaplasia, are seen in up to 60% of patients with bladder exstrophy several years post-primary closure. Although the absence of dysplasia was reported in this series, the importance of long-term follow-up in this population with unclear malignant potential was highlighted by the authors [4].
Keratinizing squamous metaplasia has been recognized as a major risk factor for bladder carcinoma. Khan, et al. studied patients with extensive keratinizing squamous metaplasia, i.e., more than 50% mucosal involvement, of whom 54% developed subsequent cancers, many with advanced disease [8]. Even patients with limited squamous metaplasia, i.e., 50% mucosal involvement, had a 12.5% chance of developing subsequent cancers. The authors concluded that patients with keratinizing squamous metaplasia require lifelong follow-up, with selected patients with extensive disease and long life expectancy being candidates for cystectomy [7,8].
The progression from chronic irritation to malignancy is a well-documented phenomenon in exstrophy patients. The presence of chronic inflammation and physical trauma, often resulting from calculi or external exposure, can trigger a protective but maladaptive response in the urothelium, leading to squamous metaplasia. While the patient exhibited non-keratinizing changes, the established association between long-standing irritation, dysplasia, and eventual squamous cell carcinoma justifies a proactive surgical approach to eliminate this oncogenic risk.
The rationale for proceeding with the radical cystectomy in this patient was multifactorial. Ko, et al. studied the outcomes of patients undergoing cystectomy in the pediatric population with exstrophy of the bladder, the most common reason being intrinsically diseased bladder templates that were too small despite interval growth, often with poor tissue quality [9]. In this patient, the rationale was the poor tissue quality, as evidenced by the recurrent fistulae, the presence of squamous metaplasia, recurrent stones, and the failure of previous reconstructive efforts.
Phelps and Malone reported an unusual complication of severe perineal pain following enterocystoplasty, which resolved with the excision of the native bladder in patients with bladder exstrophy [10]. Histological analysis of the bladder tissue revealed squamous metaplasia, leading the authors to suggest that cystectomy may cure the pain and eliminate the risk of future malignant change.
The ileal conduit procedure, as described by the Bricker technique, was an appropriate choice as a urinary diversion method in this case, as it is a well-known, simple solution that provides reliable and reproducible outcomes. Continent urinary diversion is an attractive solution that has been shown to have good results, with 93% of patients showing good continence outcomes [11]. However, this procedure is not without its risks, including the possibility of stenosis of the continent stoma (23%) and the development of stones in the diversion (26%) [3]. In this patient, with a history of failed surgical reconstructions, an ileal conduit was the best solution, as it is a reliable method with fewer long-term complication risks.
Long-term surveillance is essential in all cases of BE, whether with preservation of the bladder or diversion. In a study done by Woodhouse et al., it was found that there is a 700-fold increased risk of bladder cancer in adult exstrophy patients by the age of 40 years [5].
It is acknowledged that the transition to a definitive ileal conduit constitutes a substantial lifestyle modification for a 21-year-old male. While continent diversions offer superior psychological and continence benefits, the patient’s history of recurrent stones and poor tissue vascularity rendered the risk of pouch complications or stomal stenosis excessively high. While the 3-month outcomes are encouraging, the primary limitation of this report is the short follow-up period. Lifelong surveillance remains mandatory to monitor upper tract function and overall quality of life following such radical surgery.
The case shows that in cases of failed reconstructions, poor-quality bladders, and abnormal histological findings in BE patients, the role of radical cystectomy with urinary diversion is significant. The presence of squamous metaplasia, even in early stages, must be seriously considered, especially regarding its potential for malignancy. A multidisciplinary approach is mandatory in the management of such cases in conjunction with the urological and pathological community and the patient. Early detection of such cases that may benefit from definitive surgical management may prevent future complications and life-threatening malignancies.
Declaration
Ethical approval: Ethics approval has been obtained to proceed with the current study
Ethical approval for this study (Ethical Committee N009-24) was provided by the Ethical Committee of Ibn University Hospitals, Rabat, Morocco, on 22 January 2024
Consent: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of the journal.
Guarantor of submission: The corresponding author is the guarantor of the submission.
Availability of data and materials: Supporting material is available if further analysis is needed.
Provenance and peer review: Not commissioned, externally peer-reviewed.
- Ebert AK, Reutter H, Ludwig M, Rösch WH. The exstrophy-epispadias complex. Orphanet J Rare Dis. 2009;4:23. Available from: https://doi.org/10.1186/1750-1172-4-23
- Abdellaoui S, Cazzorla F, Morel-Journel N, Bidault V, Neuville P, Ruffion A, et al. Long-term urinary outcomes in classic bladder exstrophy: results of an extensive follow-up. BJU Int. 2025;135(6):1018-1024. Available from: https://doi.org/10.1111/bju.16680
- Maruf M, Manyevitch R, Michaud J, Jayman J, Kasprenski M, Zaman MH, et al. Urinary continence outcomes in classic bladder exstrophy: a long-term perspective. J Urol. 2020;203(1):200-205. Available from: https://doi.org/10.1097/ju.0000000000000505
- Rubenwolf PC, Eder F, Ebert AK, Hofstaedter F, Woodhouse CR, Roesch WH. Persistent histological changes in the exstrophic bladder after primary closure: a cause for concern. J Urol. 2013;189(2):671-677. Available from: https://doi.org/10.1016/j.juro.2012.08.210
- Woodhouse CR, North AC, Gearhart JP. Standing the test of time: long-term outcome of reconstruction of the exstrophy bladder. World J Urol. 2006;24(3):244-249. Available from: https://doi.org/10.1007/s00345-006-0053-7
- Kasprenski M, Michaud J, Yang Z, Maruf M, Benz K, Jayman J, et al. Urothelial differences in the exstrophy-epispadias complex: potential implications for management. J Urol. 2021;205(5):1460-1465. Available from: https://doi.org/10.1097/ju.0000000000001510
- Clouston D, Lawrentschuk N. Metaplastic conditions of the bladder. BJU Int. 2013;112 Suppl 2:27-31. Available from: https://doi.org/10.1111/bju.12378
- Khan MS, Thornhill JA, Gaffney E, Loftus B, Butler MR. Keratinising squamous metaplasia of the bladder: natural history and rationalization of management. Eur Urol. 2002;42(5):469-474. Available from: https://doi.org/10.1016/s0302-2838(02)00358-5
- Ko JS, Lue K, Friedlander D, Baumgartner T, Stuhldreher P, DiCarlo HN, et al. Cystectomy in the pediatric exstrophy population: indications and outcomes. Urology. 2018;116:168-171. Available from: https://doi.org/10.1016/j.urology.2017.09.009
- Phelps SR, Malone PS. Severe perineal pain after enterocystoplasty in bladder exstrophy. BJU Int. 2004;93(6):835-837. Available from: https://doi.org/10.1111/j.1464-410x.2003.04741.x
- Surer I, Ferrer FA, Baker LA, Gearhart JP. Continent urinary diversion and the exstrophy-epispadias complex. J Urol. 2003;169(3):1102-1105. Available from: https://doi.org/10.1097/01.ju.0000044921.19074.d0