
More Information
Submitted: June 18, 2026 | Accepted: June 22, 2026 | Published: June 24, 2026
Citation: Mikou MA, Soufiani I, Bakouch M, El-Abidi H, Ziani I, Boualaoui I, et al. Assessment of the Quality of Life in Patients Undergoing Radical Cystectomy with Urinary Diversion. J Clin Med Exp Images. 2026; 10(1): 44-49. Available from:
https://dx.doi.org/10.29328/journal.jcmei.1001048
DOI: 10.29328/journal.jcmei.1001048
Copyright license: © 2026 Mikou MA, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Radical cystectomy; Urinary diversion; Quality of life; Bladder cancer; Body image; Socioeconomic status

Assessment of the Quality of Life in Patients Undergoing Radical Cystectomy with Urinary Diversion
Mohamed Ali Mikou*, Ilyas Soufiani, Mohamed Bakouch, Hamza El-Abidi, Idriss Ziani, Imad Boualaoui, Ahmed Ibrahimi and Yassine Nouini
Urology Department A, Ibn Sina University Hospital, Rabat, Morocco
*Corresponding author: Mohamed Ali Mikou, Urology Department A, Ibn Sina University Hospital, Rabat, Morocco, Email: [email protected]
Radical cystectomy with urinary diversion is the standard treatment for muscle-invasive bladder cancer. The impact of the type of urinary diversion on quality of life (QoL) remains debated. This cross-sectional study assessed QoL in 57 patients who underwent radical cystectomy between 2014 and 2022 at two urology departments in Rabat, Morocco, using the Bladder Cancer Index (BCI), the SF-36, and the Body Image Scale (BIS). Multiple linear regression identified socioeconomic status, body image perception, urinary discomfort, and comorbidities as the main determinants of QoL, with the type of urinary diversion playing an indirect role mediated through these factors. These findings underscore the need for a multidimensional approach when evaluating and optimizing QoL outcomes after radical cystectomy.
Radical cystectomy with urinary diversion is the gold standard treatment not only for muscle-invasive bladder cancers classified as T2–T4N0M0, but also for very high-risk superficial tumors, BCG therapy-resistant forms, and tumors that cannot be controlled endoscopically.
The procedure is often perceived by patients as a traumatic event with major repercussions on urinary and sexual function, inducing psychosocial stress secondary to a change in body image.
The World Health Organization defines quality of life as ‘the person’s physical health, psychological state, level of independence, social relationships and their relationship to salient features of their environment’ [1]. Quality of life is of the utmost importance, as its reduction can itself influence survival [2,3].
Several types of urinary diversion have been designed in an attempt to minimize complications and optimize post-operative quality of life, most using the bowel to reconstruct the urinary tract.
Consequently, understanding the different urinary diversion options with their respective impact on quality of life is essential to informed consent and should be captured in data acquired from rigorous scientific investigation.
The aim of this study is to assess the quality of life of patients who underwent urinary diversion after radical cystectomy and to identify the different parameters that may have an impact on each of its aspects.
Data were collected from the archives of the years 2014 to 2022 of the Urology Department A of the Ibn Sina University Hospital and the Urology Department of the Mohammed V Military Training Hospital in Rabat.
Patients included in this study were reachable individuals aged over 18 years who had undergone radical cystectomy for bladder cancer between 2014 and 2022 in the two aforementioned departments and who were able to complete the questionnaires independently.
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and received approval from the Institutional Ethics Committee of Ibn Sina University Hospital, Rabat. Given the retrospective, archive-based identification of eligible patients, medical record review was conducted on anonymized data. All patients subsequently contacted for questionnaire completion were informed of the purpose of the study and of the voluntary, confidential nature of their participation, and provided informed consent prior to completing the questionnaires.
Quality of life was assessed using several complementary validated questionnaires.
Bladder Cancer Index (BCI)
Developed and validated at the University of Michigan by Gilbert, et al. in 2010, this questionnaire is designed to measure quality of life specifically in patients with bladder cancer and/or urinary diversions (orthotopic neobladder or trans-ileal Bricker-type ileal conduit) [4]. It is available and validated in several languages, including Arabic [5]. The BCI comprises 34 items divided into three main domains measuring urinary, sexual, and bowel functions, each with two sub-domains (function and discomfort). For ileal conduit patients, the BCI additionally measures stoma and appliance function, leakage, and skin irritation. Responses are based on a Likert scale, and composite scores are standardized on a 0–100 scale, with higher scores indicating better function.
Table 1 summarizes the domains, sub-domains, and scoring principles of the BCI.
| Table 1: Summary of the Bladder Cancer Index (BCI) domains, sub-domains, and scoring. | |||
| Domain | Sub‑domain | Content Assessed | Score Range |
| Urinary | Function (FU) | Continence, voiding control, urinary habits | 0–100 |
| Discomfort (GU) | Bother/distress caused by urinary symptoms | 0–100 | |
| Bowel | Function (FD) | Bowel habits and digestive symptoms | 0–100 |
| Discomfort (GD) | Bother/distress caused by digestive symptoms | 0–100 | |
| Sexual | Function (FS) | Sexual desire, performance, satisfaction | 0–100 |
| Discomfort (GS) | Bother/distress related to sexual function | 0–100 | |
| Stoma/Appliance¹ | Function | Appliance management, leakage, peristomal skin irritation (ileal conduit patients only) | 0–100 |
| ¹ Assessed only in patients with a Bricker-type ileal conduit. Higher scores indicate better function/less bother. Adapted from Gilbert et al., 2010 [4]. | |||
RAND SF-36 health survey
The SF-36 is the most established and widely used general quality of life assessment tool, and has been translated and validated in Arabic [6]. This questionnaire comprises 36 questions across eight functional domains: physical functioning, role limitations due to physical problems, role limitations due to emotional problems, energy and fatigue, emotional well-being, social functioning, bodily pain, and general health. Scores for each dimension are combined to yield an overall quality of life score.
Table 2 summarizes the dimensions and item composition of the SF-36.
| Table 2: Summarizes the dimensions and item composition of the SF-36. | ||
| Domain | Items (n) | Content Assessed |
| Physical Functioning | 10 | Limitations in physical activities (e.g., walking, climbing stairs, lifting) |
| Role Limitations – Physical | 4 | Limitations in usual activities due to physical health problems |
| Role Limitations – Emotional | 3 | Limitations in usual activities due to emotional problems |
| Energy/Fatigue (Vitality) | 4 | Level of energy versus fatigue |
| Emotional Well‑Being (Mental Health) | 5 | Psychological distress and well‑being |
| Social Functioning | 2 | Impact of health on social activities |
| Bodily Pain | 2 | Intensity of pain and its interference with activities |
| General Health | 5 | Personal perception of overall health status |
| Each domain is scored from 0 to 100, with higher scores indicating better health status; a remaining single item assesses perceived health transition and is not included in the eight domain scores. Adapted from Ware & Sherbourne and the RAND scoring protocol [6]. | ||
Each domain is scored from 0 to 100, with higher scores indicating better health status; a remaining single item assesses perceived health transition and is not included in the eight domain scores. Adapted from Ware & Sherbourne and the RAND scoring protocol [6].
Body Image Scale (BIS)
Developed by Hopwood, et al., the BIS is a concise 10-item questionnaire validated in French that focuses on patients’ affective and behavioral experience of their body image specifically as a result of cancer and its treatment, including aspects related to physical appearance, bodily integrity, and feelings of attractiveness [7].
Socioeconomic status
To stratify the population by socioeconomic level, three criteria were used: one subjective criterion (self-ranking of household social level relative to the immediate environment) and two objective criteria based on household income and living standards (expenditures). Socioeconomic status was additionally quantified using a validated score developed by Sawsan I. Fahmy, et al. in 2015 at the University of Alexandria, Egypt — a country culturally and economically close to Morocco.
Statistical analysis
Statistical analysis was performed using JAMOVI software (version 2.3.21). Quantitative variables were described as mean ± standard deviation or median and interquartile range, depending on the distribution. Qualitative variables were described as counts and percentages.
Multiple linear regression was used to assess predictors of quality of life scores. Predictors included urinary diversion type, socioeconomic status, current age, age at surgery, interval (in months) between surgery and questionnaire completion, smoking status, presence or absence of comorbidities, tumor invasion stage, and body image score (BIS). Urinary discomfort measured by the BCI was additionally included as a predictor at the SF-36 domain level. Pairwise comparison was used to identify significant differences between groups.
A total of 215 cystectomies were performed during the study period, of which 57 patients met the inclusion criteria (51 men and 6 women). The mean age at cystectomy was 64.12 years (range: 49–82 years). The mean age at the time of the study was 66.49 years. The average interval between surgery and questionnaire completion was 28 months.
Ten patients had a low socioeconomic status, and eight had a high one. Further patient characteristics are summarized in Table 3.
| Table 3: Baseline demographic and clinical characteristics of the study population (n = 57). | ||||||
| Category | Sub‑group | Number | Percentage (%) | Actual age (ans) | Age at cystectom (ans) | interval (mois) |
| Patient sex | Male | 51 | 89,47 | 66,33 | 63,80 | 35,22 |
| Female | 6 | 10,53 | 69,33 | 66,83 | 37,00 | |
| Type de dérivation urinaire | Type of urinary diversion | 11 | 19,30 | 66,18 | 63,45 | 37,64 |
| Cutaneous ureterostomy | 20 | 35,09 | 64,15 | 61,50 | 37,75 | |
| Ileal conduit (Bricker) | 26 | 45,61 | 68,77 | 66,42 | 32,65 | |
| Socio-economic status | Bas | 10 | 17,54 | 66,60 | 65,00 | 24,60 |
| Average | 39 | 68,42 | 66,05 | 63,56 | 34,97 | |
| High | 8 | 14,04 | 69,63 | 65,75 | 51,00 | |
| Invasion of the wall | TVIM | 47 | 82,46 | 65,77 | 63,23 | 35,49 |
| TV/NIM | 10 | 17,54 | 70,80 | 68,30 | 35,00 | |
| Histological type | Urothelial carcinoma | 57 | 100,00 | — | — | — |
| Other | 0 | 0,00 | — | — | — | |
Men had higher BCI scores in the function sub-domains (urinary, digestive, and sexual), while women had higher scores in the discomfort sub-domains (urinary, digestive, and sexual), across the three types of urinary diversion (orthotopic neobladder, Bricker ileal conduit, and cutaneous ureterostomy), as described in Table 4 and Figure 1.
| Table 4: BCI sub-domain averages by urinary diversion type. | ||||
| Category | Measure | Bladder replacement ± SD | Ileal conduit (Bricker) ± SD | Cutaneous urethrostomy ± SD |
| Urinaire | Fonction | 34.20 (± 25) | 74.99 (± 17) | 76.67 (± 15) |
| Gêne | 79.55 (± 23) | 76.63 (± 23) | 81.88 (± 18) | |
| Digestive | Fonction | 73.30 (± 10) | 77.49 (± 9) | 73.54 (± 12) |
| Gêne | 75.00 (± 15) | 77.72 (± 12) | 82.50 (± 3) | |
| Sexuelle | Fonction | 32.25 (± 23) | 27.86 (± 17) | 30.79 (± 22) |
| Gêne | 41.65 (± 37) | 39.81 (± 17) | 56.50 (± 24) | |
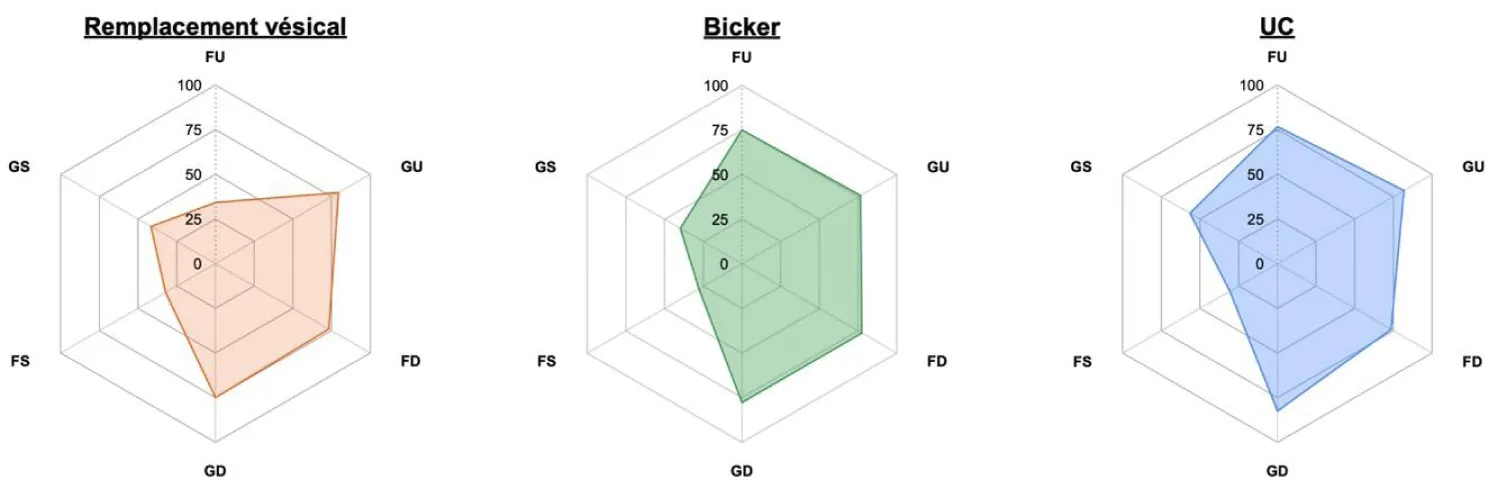
Figure 1: BCI sub-domains by urinary diversion type. FU: Urinary Function; GU: Urinary Discomfort; FD: Digestive Function; GD: Digestive Discomfort; FS: Sexual Sunction; GS: Sexual Discomfort
Women had lower SF-36 scores than men in most sub-domains. Regarding body image, Bricker patients had higher BIS scores compared to the other groups.
In terms of overall quality of life, patients with orthotopic neobladder (enterocystoplasty) had the highest scores in almost all SF-36 domains, in contrast to patients with cutaneous ureterostomy, who had the lowest scores (Figure 2).
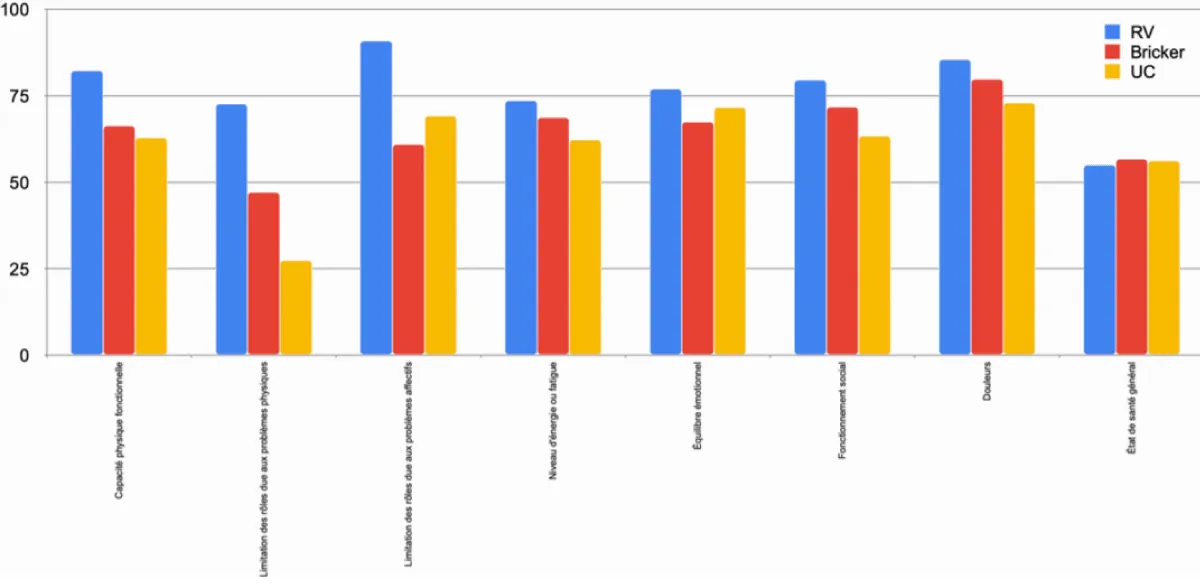
Figure 2: SF-36 domain scores by urinary diversion type.
Patients with higher socioeconomic status scored higher on both the BCI and SF-36 surveys (Figure 3). However, the perception of body image was similar across the three socioeconomic classes.
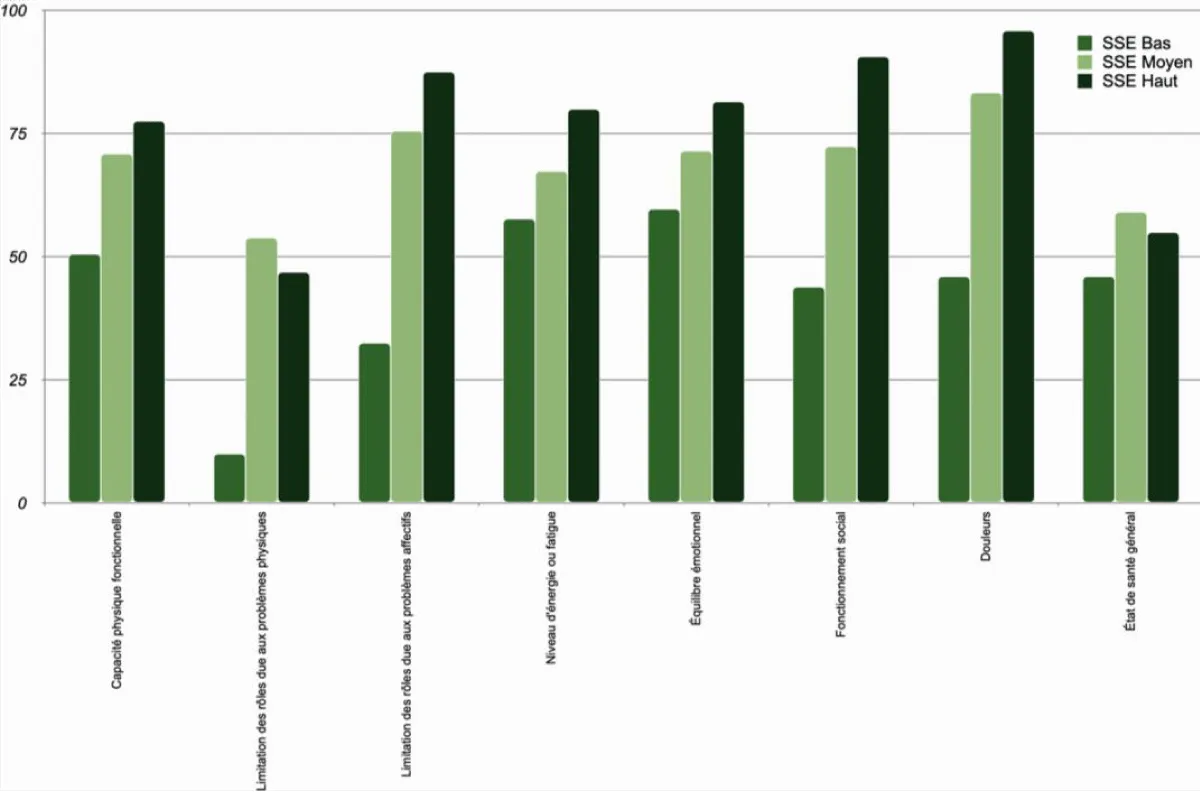
Figure 3: SF-36 domain scores by socioeconomic status.
Urinary function and discomfort tended to improve with increasing time since surgery (Figure 4). Furthermore, non-smokers had higher scores than smokers in the BCI, whereas smokers had higher scores in the SF-36, a finding attributed to confounding by higher socioeconomic status and fewer comorbidities among smokers in this cohort.
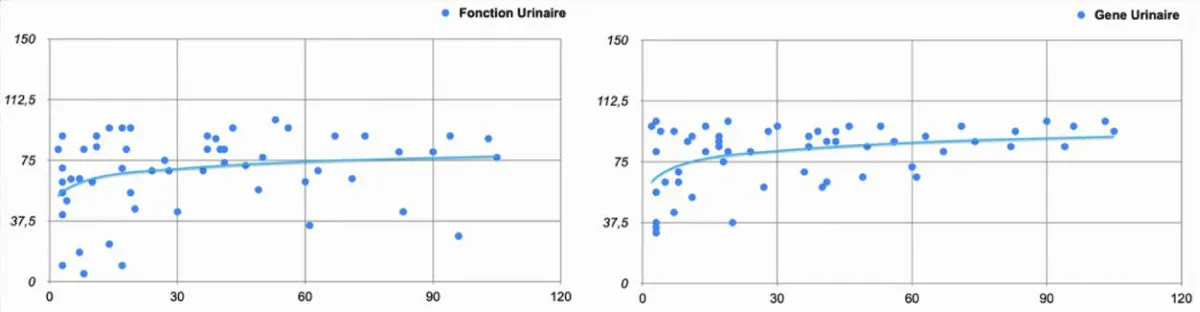
Figure 4: Urinary function and discomfort by interval between cystectomy and assessment (months).
Factors predicting quality of life scores
Multiple linear regression analysis identified the following predictors of quality of life:
A. Bladder Cancer Index (BCI)
Urinary function: Type of urinary diversion (F = 36.11, p < 0.001), socioeconomic status (F = 5.09, p = 0.010), and interval between cystectomy and assessment (F = 4.31, p = 0.043).
Urinary discomfort: Socioeconomic status (F = 9.51, p < 0.001), BIS score (F = 8.27, p = 0.006), and interval between cystectomy and evaluation (F = 9.03, p = 0.004).
Digestive function: BIS score (F = 4.49, p = 0.039) and tumor invasion stage (F =4.29, p = 0.043).
Digestive discomfort: Socioeconomic status (F = 7.39, p = 0.007), type of urinary diversion (F = 3.59, p = 0.035), and smoking status (F = 4.42, p = 0.041).
Sexual function: Interval between cystectomy and assessment (F = 6.42, p = 0.014), BIS score (F = 4.62, p = 0.036), and age at cystectomy (F = 4.44, p = 0.040).
Sexual discomfort: Sex (F = 9.44, p = 0.003) and smoking status (F = 5.81, p = 0.019).
B. SF-36 Questionnaire
Physical functioning: Urinary discomfort (F = 6.00, p = 0.018).
Role limitations – physical: Urinary discomfort (F = 19.81, p < 0.001), type of urinary diversion (F = 4.86, p = 0.012), and smoking status (F = 6.54, p = 0.014).
Role limitations-emotional: BIS score (F = 13.30, p < 0.001), socioeconomic status (F = 5.35, p = 0.008), and smoking status (F = 4.55, p = 0.038).
Energy and fatigue: Urinary discomfort (F = 17.78, p < 0.001) and presence of comorbidities (F = 9.71, p = 0.003).
Emotional well-being: Socioeconomic status (F = 7.64, p = 0.008), BIS score (F = 10.76, p = 0.002), presence of comorbidities (F = 10.46, p = 0.002), and current age (F = 6.71, p = 0.012).
Social functioning: Socioeconomic status (F = 11.66, p = 0.001), urinary discomfort (F = 14.02, p < 0.001), and presence of comorbidities (F = 17.25, p < 0.001).
Bodily pain: Current age (F = 6.18, p = 0.016) and socioeconomic status (F = 13.54, p < 0.001).
General health: Urinary discomfort (F = 5.34, p = 0.025) and presence of comorbidities (F = 7.43, p = 0.009).
C. Body Image Perception (BIS)
Type of urinary diversion (F = 4.46, p = 0.016) and sexual embarrassment (F = 7.95, p = 0.007). Notably, having a stoma did not exert a significant effect on body image perception; significant differences in pairwise comparison were observed between patients with Bricker ileal conduit and those with the other two urinary diversion types.
D. Socioeconomic Status
Age at cystectomy (F = 4.26, p = 0.044), type of urinary diversion (F = 8.27, p < 0.001), and urinary discomfort (F = 17.91, p < 0.001).
In recent years, the impact of disease and treatment on patients’ physical, psychological, and social functioning has become central to the therapeutic decision-making process. Consequently, health-related quality of life after urinary diversion has been increasingly recognized as an important outcome measure.
Numerous studies have attempted to address this topic using different questionnaires and assessing multiple factors, including the type of urinary diversion, while often neglecting other determinants. The present study sought to take a more holistic view.
Due to the small number of female patients in this cohort, a statistical comparison between sexes was not performed.
According to the BCI, the type of urinary diversion had a statistically significant effect only on the domains of urinary function and digestive discomfort.
Patients who underwent orthotopic neobladder reconstruction had a significantly lower urinary function score than those with other types of urinary diversion, but a better perception of body image. These results are consistent with those of previous studies using the same assessment instrument [4,8–11]. This is likely attributable to the persistence of daytime incontinence (82%), and particularly nocturnal incontinence (100%).
However, as demonstrated in various cohorts [12,13], urinary function and discomfort improve with increasing time since cystectomy, suggesting that patients adapt over time to different functional alterations regardless of the type of urinary diversion.
On the digestive side, constipation was the most frequent problem but tended to improve over time. Regardless of the type of urinary diversion, it was not severe enough to exert a statistically significant effect on the digestive function domain of the BCI; however, digestive discomfort was more frequently reported with orthotopic neobladder reconstruction.
In this series, only 19.3% of patients were sexually active, mainly due to erectile dysfunction. The most decisive factor for sexual function and discomfort was body image perception as measured by the BIS, consistent with the literature [12–16], and in particular the feeling of diminished masculinity or femininity, which is closely linked to sexual performance in many cultural contexts. Sexual function improved over time, though not to preoperative levels [12].
With regard to the general quality of life as measured by the SF-36, patients with orthotopic neobladder had the highest scores in almost all domains, followed by Bricker patients, and then patients with cutaneous ureterostomy. These results are consistent with the literature, which shows no statistically significant difference by diversion type [17]. In contrast, other parameters identified by multiple linear regression — specifically socioeconomic status, BIS score, presence of comorbidities, and urinary discomfort — were significant predictors of SF-36 scores [18–22].
A notable finding was that smokers had higher scores in most SF-36 domains, while nonsmokers had better BCI functional outcomes. This paradoxical result is attributable to confounding, as smokers in this cohort had, on average, higher socioeconomic status and fewer comorbidities.
Limitations
This study has several limitations. First, the small sample size may have contributed to selection bias. Second, only six women were included, precluding a separate gender analysis, although our results are consistent with those of studies using similar assessment instruments. Third, the study was conducted in a public hospital setting, where the patient population may not be fully representative of the general population. Fourth, the cross-sectional design limits the ability to assess the longitudinal evolution of quality of life. Finally, residual confounding from unmeasured variables cannot be excluded. Prospective studies and randomized controlled trials conducted within our sociocultural context would be valuable to better characterize the various parameters examined here.
This study was conducted on the hypothesis that quality of life after radical cystectomy with urinary diversion is determined not solely by the type of diversion itself, but by a broader, multidimensional set of factors — including socioeconomic status, body image perception, urinary discomfort, and comorbidities — through which the type of diversion may exert an indirect rather than a direct effect. The findings of this study corroborate this hypothesis: multivariate analysis did not identify a direct effect of the type of urinary diversion on overall quality of life, but rather an indirect effect mediated through its associations with socioeconomic status and perceived body image, which emerged as the most important determinants of both general and bladder cancer-specific health-related quality of life. Although patients who underwent orthotopic neobladder reconstruction had favorable scores in several domains, this advantage did not translate into a statistically independent effect of diversion type on overall quality of life once these mediating factors were accounted for.
The type of urinary diversion did, however, have a direct effect on urinary function as measured by the BCI. Urinary discomfort was similar across the three diversion types and itself emerged as a significant predictor of multiple SF-36 domains.
These findings underscore the need for a multidimensional approach when assessing quality of life outcomes in bladder cancer patients undergoing radical cystectomy. Further research is warranted to better understand the mechanisms underlying these associations and to develop targeted interventions aimed at improving health outcomes in this population.
- World Health Organization. WHOQOL – Measuring Quality of Life. Available from: https:// www.who.int/tools/whoqol
- Coates A, Porzsolt F, Osoba D. Quality of life in oncology practice: Prognostic value of EORTC QLQ-C30 scores in patients with advanced malignancy. Eur J Cancer. 1997;33(7):1025–1030. Available from: https://doi.org/10.1016/s0959-8049(97)00049-x
- Roychowdhury DF, Hayden A, Liepa AM. Health-related quality-of-life parameters as independent prognostic factors in advanced or metastatic bladder cancer. J Clin Oncol. 2003;21(4):673–678. Available from: https://doi.org/10.1200/jco.2003.04.166
- Gilbert SM, Dunn RL, Hollenbeck BK, Montie JE, Lee CT, Wood DP, et al. Development and validation of the Bladder Cancer Index: a comprehensive, disease-specific measure of health-related quality of life in patients with localized bladder cancer. J Urol. 2010;183(5):1764–1770. Available from: https://doi.org/10.1016/j.juro.2010.01.013
- Ziouziou I, Touzani MA, Karmouni T. Arabic translation and linguistic validation of the Bladder Cancer Index questionnaire. Afr J Urol. 2018;24(2):104–107.
- Brazier JE, Harper R, Jones NM, O'Cathain A, Thomas KJ, Usherwood T, et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ. 1992;305(6846):160–164. Available from: https://doi.org/10.1136/bmj.305.6846.160
- Hopwood P, Fletcher I, Lee A, Al Ghazal S. A body image scale for use with cancer patients. Eur J Cancer. 2001;37(2):189–197. Available from: https://doi.org/10.1016/s0959-8049(00)00353-1
- Goldberg H, Baniel J, Mano R, Rotlevy G, Kedar D, Yossepowitch O. Orthotopic neobladder vs. ileal conduit urinary diversion: a long-term quality-of-life comparison. Urol Oncol. 2016;34(3):121.e1–121.e7. Available from: https://doi.org/10.1016/j.urolonc.2015.10.006
- Gellhaus PT, Cary C, Kaimakliotis HZ, Johnson CS, Weiner M, Koch MO, et al. Long-term health-related quality of life outcomes following radical cystectomy. Urology. 2017;106:82–86. Available from: https://doi.org/10.1016/j.urology.2017.03.053
- Héver NV, Péntek M, Balló A, Gulácsi L, Baji P, Brodszky V, et al. Health-related quality of life in patients with bladder cancer: a cross-sectional survey and validation study of the Hungarian version of the Bladder Cancer Index. Pathol Oncol Res. 2015;21(3):619–627. Available from: https://doi.org/10.1007/s12253-014-9866-7
- Osawa T, Wei JT, Abe T, Honda M, Yamada S, Furumido J, et al. Health-related quality of life in Japanese patients with bladder cancer measured by a newly developed Japanese version of the Bladder Cancer Index. Int J Clin Oncol. 2020;25(12):2090–2098. Available from: https://doi.org/10.1007/s10147-020-01770-2
- Clements MB, Atkinson TM, Dalbagni GM, Li Y, Vickers AJ, Herr HW, et al. Health-related quality of life for patients undergoing radical cystectomy: results of a large prospective cohort. Eur Urol. 2022;81(3):294–304. Available from: https://doi.org/10.1016/j.eururo.2021.09.018
- Huang Y, Pan X, Zhou Q, Huang H, Li L, Cui X, et al. Quality-of-life outcomes and unmet needs between ileal conduit and orthotopic ileal neobladder after radical cystectomy in a Chinese population: a 2to-1 matched-pair analysis. BMC Urol. 2015;15(1):117. Available from: https://doi.org/10.1186/s12894-015-0113-7
- Herrel L, Umarji R, Lee C. Sexual function changes in bladder cancer patients undergoing cystectomy. J Urol. 2015;193(4S):e520.
- Min C, Qiang L, Feifan W. Sexual function in males after radical cystectomy. J Sex Med. 2018;15(Suppl 3):S293.
- Hedgepeth RC, Gilbert SM, He C, Lee CT, Wood DP. Body image and bladder cancer-specific quality of life in patients with ileal conduit and neobladder urinary diversions. Urology. 2010;76(3):671–675. Available from: https://doi.org/10.1016/j.urology.2010.01.087
- Shi H, Yu H, Bellmunt J, et al. Comparison of health-related quality of life (HRQoL) between ileal conduit diversion and orthotopic neobladder based on validated questionnaires: a systematic review and meta-analysis. Qual Life Res. 2018;27(11):2759–2775. Available from: https://doi.org/10.1007/s11136-018-1902-8
- Nayir T, Uskun E, Yürekli MV, Leow JJ, Chen X, Guo C, et al. Does body image affect quality of life? A population-based study. PLoS ONE. 2016;11(9):e0163290. Available from: https://doi.org/10.1007/s11136-018-1902-8
- Chow KM, Chan CWH, Leung AWY, Wong MMH, Choi KC. Relationship between body image and health-related quality of life in Chinese cancer survivors during the transitional cancer survivorship period. Psychooncology. 2019 Feb;28(2):324-328. Available from: https://doi.org/10.1002/pon.4943
- Teo I, Cheung YB, Lim TYK, Namuduri RP, Long V, et al. The relationship between symptom prevalence, body image, and quality of life in Asian gynecologic cancer patients. Psychooncology. 2018 Jan;27(1):69-74. Available from: https://doi.org/10.1002/pon.4457
- Henry M, Ho A, Lambert SD, Carnevale FA, Greenfield B, MacDonald C, et al. Looking beyond disfigurement: the experience of patients with head and neck cancer. J Palliat Care. 2014;30(1):5–15.
- Rhoten BA, Murphy B, Ridner SH. Body image in patients with head and neck cancer: a review of the literature. Oral Oncol. 2013;49(8):753–760. Available from: https://doi.org/10.1016/j.oraloncology.2013.04.005